![The Zero Trimester Trend: Why Women Are Training for Pregnancy [2025]](https://tryrunable.com/blog/the-zero-trimester-trend-why-women-are-training-for-pregnanc/image-1-1770205059731.jpg)
The Zero Trimester Movement: More Than Just Wellness Hype
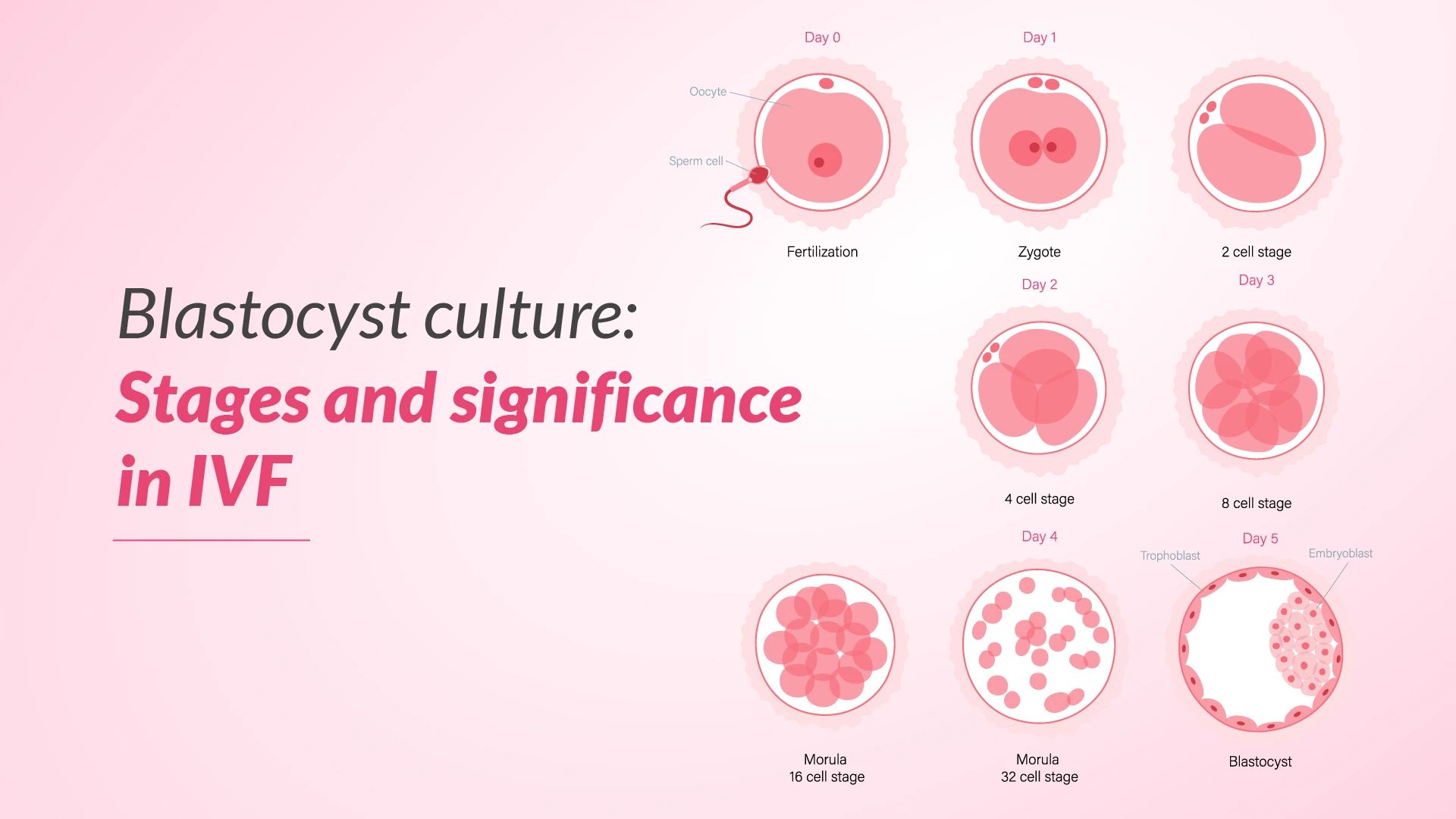
Three years of meticulous planning. Raw milk cleanses. Sunset gazing for circadian optimization. Mercury detoxification protocols costing hundreds of dollars. Specialized pelvic floor Pilates courses. Hormone testing through light-frequency hand scans.
This isn't the setup for a wellness retreat or a high-end spa package. This is what some women are doing to prepare for pregnancy—not when they're actively trying to conceive, but months or even years before they've decided to have a baby at all.
Welcome to the "zero trimester," a concept that's blurred the line between reasonable preconception health and an increasingly elaborate wellness obsession that's reshaping how millions of women think about their fertility, their bodies, and what they owe their future children before those children even exist.
The trend has quietly exploded across social media. Instagram hashtags like #preconception have accumulated over 106,000 posts. TikTok videos tagged #pregnancyprep regularly rack up millions of views, with some creators boasting seven-figure follower counts dedicated entirely to this niche. Search trends show a 345% increase in Google searches for "pregnancy preparation" over the past five years, with spikes in January—the traditional "new year, new me" season—suggesting this isn't a fleeting trend but a deeply embedded cultural moment.
What makes this movement particularly significant—and troubling to some medical professionals—is how it weaponizes the language of empowerment and choice. "Healthy pregnancy isn't chance—it's choice," has become the rallying cry of the zero trimester influencer sphere. The message resonates powerfully: You're not at the mercy of genetics or bad luck. You can control your outcome. You can optimize yourself into a perfect pregnancy if you just follow the formula.
But what's the actual evidence behind these protocols? Who's profiting from this wellness arms race? And what happens when the promise of total control meets the unpredictable reality of human biology?
TL; DR
- Growing Movement: The "zero trimester" concept has spawned a $2+ billion wellness industry focused on preconception optimization
- Influencer-Driven: TikTok and Instagram creators with millions of followers are promoting unproven fertility protocols and pricey supplements
- Mixed Science: While some preconception health measures (folic acid, exercise, stress reduction) have solid evidence, most "biohacking" strategies lack rigorous clinical validation
- Access Issues: Premium pregnancy prep courses, specialized testing, and recommended supplements create a two-tiered fertility system based on wealth
- Psychological Cost: The pressure to optimize every biological parameter is contributing to anxiety, perfectionism, and unrealistic expectations around conception and pregnancy
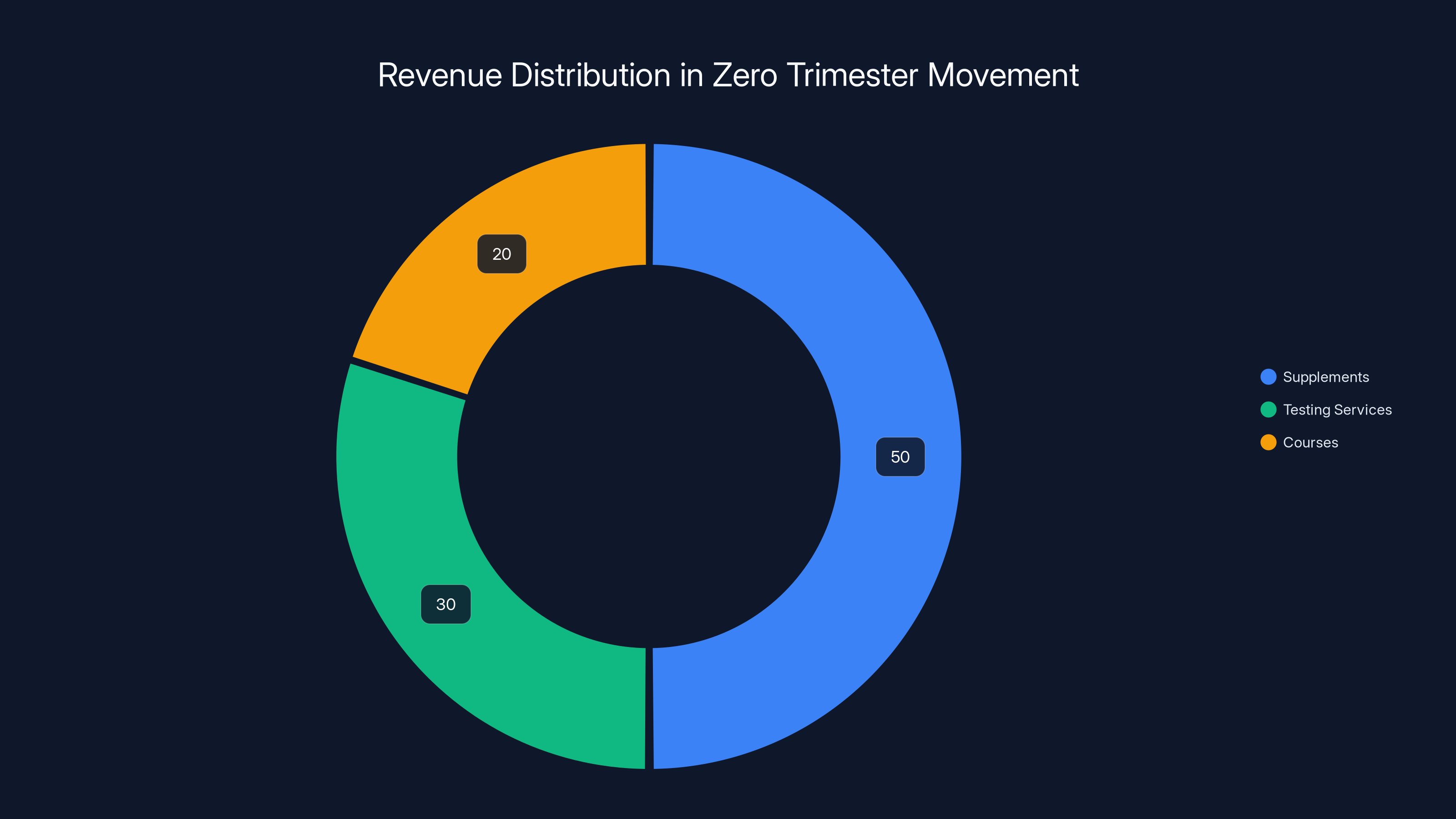
Estimated data shows supplements dominate the revenue share at 50%, followed by testing services at 30%, and courses at 20%. This highlights the significant financial impact of supplements in the zero trimester movement.
Understanding the Zero Trimester: Where a Concept Became a Culture
The term "zero trimester" itself isn't new. Sociologist Miranda Waggoner coined it in her 2017 book, using it to describe the medically recognized preconception period when women's health decisions can influence pregnancy outcomes. The American College of Obstetricians and Gynecologists has recommended preconception health optimization since the early 1980s, and folic acid supplementation before and during pregnancy has been standard medical guidance since the 1990s for preventing neural tube defects.
So the concept of preparing your body before pregnancy has legitimate roots in clinical medicine. The problem isn't preconception health itself. The problem is what happens when that concept gets remixed through wellness culture, influencer marketing, and the broader cultural obsession with biohacking and optimization.
Traditional preconception health was straightforward: take prenatal vitamins with folic acid, maintain a healthy weight, reduce alcohol consumption, manage chronic conditions like diabetes or hypertension, and get screenings for sexually transmitted infections. These interventions had clinical evidence behind them. You didn't need to spend money you didn't have. You didn't need to overhaul your entire life.
The modern zero trimester movement, however, operates on a different logic entirely. It's borrowed the optimization mentality from the male biohacking sphere—think Bryan Johnson's "Blueprint" protocol or the quantified self movement—and applied it specifically to female reproductive capacity. The underlying assumption is that your body is a system with thousands of optimization levers, and if you pull enough of them, you'll achieve the desired outcome.
This creates a particular kind of pressure. It transforms pregnancy from something that might happen to you into something you must actively engineer. It suggests that if something goes wrong—if you struggle to conceive, if you have a complicated pregnancy, if your baby has health issues—it's not just bad luck or biology. It's because you didn't optimize hard enough.
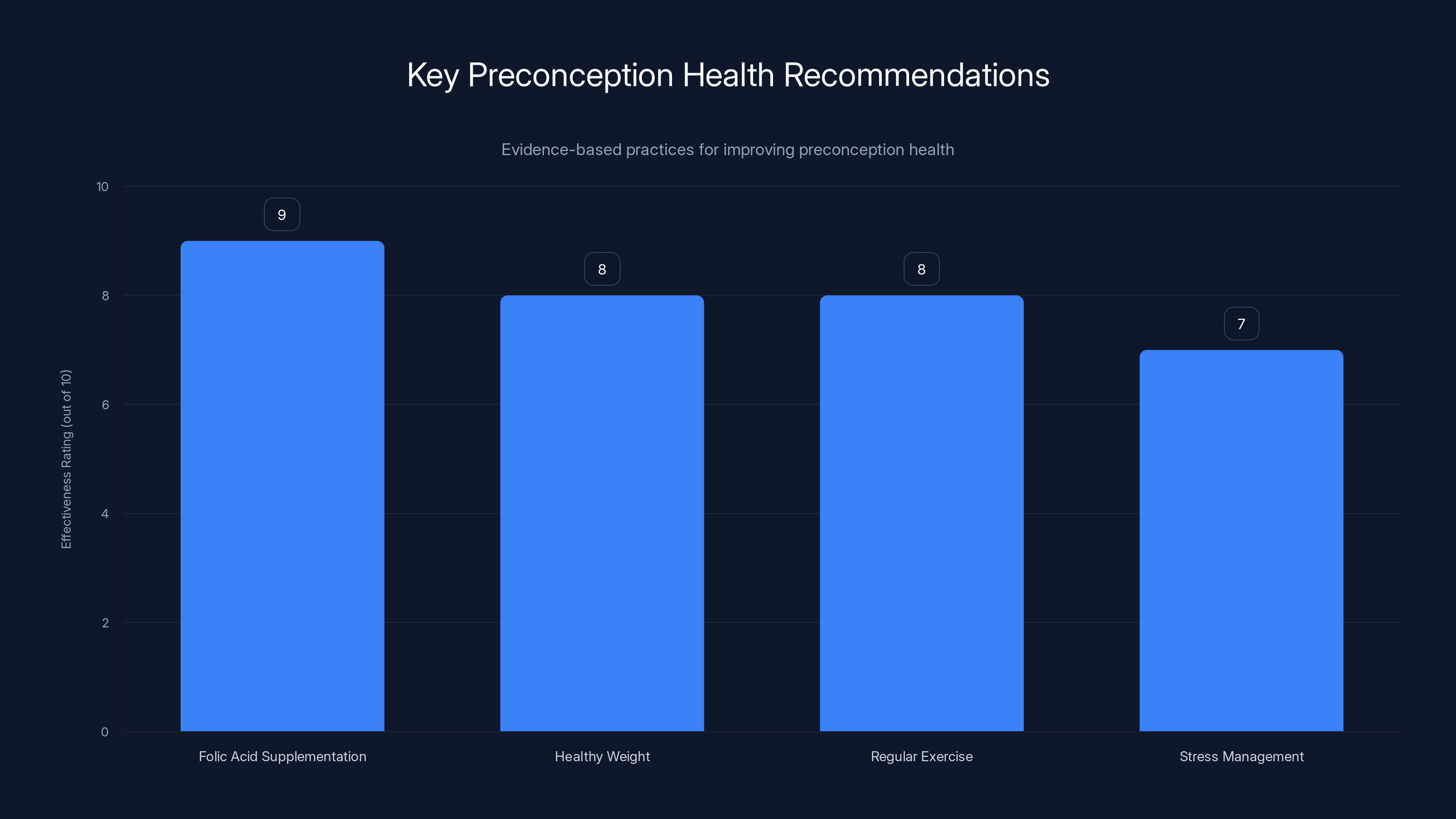
Folic acid supplementation is highly effective in reducing neural tube defects, while maintaining a healthy weight and regular exercise contribute significantly to better pregnancy outcomes. Stress management is also crucial for fertility and pregnancy health.
The Influencers Building an Empire on Preconception Anxiety
If the zero trimester has exploded as a cultural phenomenon, the credit goes to a specific cohort of influencers, functional nutritionists, health coaches, and "women's wellness experts" who've identified a massive market opportunity: millions of women worried about their fertility, their bodies, and their future as mothers.
These creators operate with remarkable consistency. They typically have six-figure to seven-figure followings. They've usually experienced their own fertility struggles or difficult pregnancies that they've reframed as personal missions to decode "the truth" about reproductive health. They present themselves as having discovered what mainstream medicine supposedly won't tell you. They speak with absolute certainty about biological mechanisms that are still actively being researched. And they sell.
Many run their own supplement lines, online courses, or branded lifestyle products. Others have affiliate relationships with supplement companies, wellness platforms, or specialized testing services. The incentive structure is transparent: more followers equals more reach for the products they're promoting, which means higher commissions or revenue from their own brands.
What's particularly effective about these creators is their aesthetic and tone. They're not selling fear; they're selling empowerment. Their content typically features glowing, happy women in beautiful settings, sipping adaptogenic coffee, journaling about their fertility intentions, or performing pelvic floor Pilates in tastefully decorated home gyms. The message is: This is what health and control look like. And it's attainable for you.
They use language that sounds grounded in biology and science. Terms like "egg health," "cellular optimization," "hormonal balance," and "reproductive toxins" pepper their captions. They cite studies (sometimes accurately, sometimes not), reference functional medicine practitioners, and share testimonials from followers who claim the protocols helped them conceive. The overall effect is authoritative without being coldly clinical. It feels like a girlfriend giving you advice, not a salesperson making a pitch.
Many of these influencers aren't doctors. Some are functional nutritionists or health coaches with minimal formal training. Others have legitimate credentials but operate outside mainstream medical guidelines. A few are nurse practitioners or registered dietitians, which provides some credibility but doesn't necessarily mean their recommendations align with evidence-based medicine. The problem is that followers often can't distinguish between these credential levels and may assume all advice comes from equivalent expertise.
The financial incentives matter. A successful pregnancy prep influencer earning income through supplements, courses, and affiliate relationships has every reason to keep expanding the protocol—add more supplements, recommend more testing, suggest longer "detoxification" periods. The more elaborate the system, the more hooks for monetization.

What the Science Actually Says About Preconception Health
Here's where things get complicated. Because buried underneath the marketing, the misinformation, and the optimization obsession, there actually is legitimate science about preconception health. The problem is that the scientific evidence gets cherry-picked, exaggerated, or completely fabricated to support the zero trimester narrative.
Let's start with what's genuinely evidence-based. Folic acid supplementation before and during pregnancy reduces the risk of neural tube defects like spina bifida by approximately 70%. This isn't controversial. Every major medical organization recommends it. Women of reproductive age should be getting at least 400 micrograms daily from supplements or fortified foods.
Maintaining a healthy weight before pregnancy is associated with better outcomes. Women with a BMI below 30 have lower rates of miscarriage, gestational diabetes, and complications during labor. But this doesn't mean extreme dieting or "optimization." It means sustainable lifestyle habits—the kind that would be beneficial whether or not pregnancy was on the horizon.
Exercise before pregnancy is beneficial. A 2021 meta-analysis found that women who engage in regular physical activity have lower rates of gestational diabetes and preeclampsia. But again, the recommendations are straightforward: 150 minutes of moderate-intensity aerobic activity per week, plus strength training. You don't need specialized pelvic floor Pilates or pregnancy-specific fitness protocols. Regular exercise works.
Managing stress and mental health matters. Chronic stress and untreated depression or anxiety can affect fertility and pregnancy outcomes. But the solution isn't watching sunrises as "antioxidant therapy." It's actual clinical mental health support—therapy, medication if needed, reasonable lifestyle modifications.
Reducing environmental toxins is reasonable in moderation. If you're using nonstick cookware, gradually replacing it with stainless steel or cast iron is a fine idea. Using personal care products without phthalates is sensible. But the obsessive elimination of every potential endocrine disruptor, the replacement of LED bulbs with incandescent lights, the removal of Wi-Fi routers from bedrooms because of "cellular health concerns"—this moves beyond evidence into anxiety-driven extremism.
Here's the critical distinction: evidence-based preconception health operates on known mechanisms with measurable risk reduction. Folic acid prevents a specific birth defect through a understood biological pathway. Exercise reduces gestational diabetes risk through metabolic mechanisms we understand. These interventions have been tested in large populations and shown to work.
Most zero trimester protocols, by contrast, operate on theoretical mechanisms with unproven benefit. The idea that watching sunrise for "antioxidant therapy" improves egg quality lacks rigorous evidence. The promise that Oligo Scans (which measure supposed mineral and heavy metal content through light-frequency hand scanning) can identify problems requiring months of chelation therapy isn't supported by clinical research. The claim that a specific supplement protocol can meaningfully improve fertility outcomes in women without diagnosed fertility issues hasn't been demonstrated in well-designed studies.
Yet these unproven interventions often command premium pricing. Oligo Scans cost
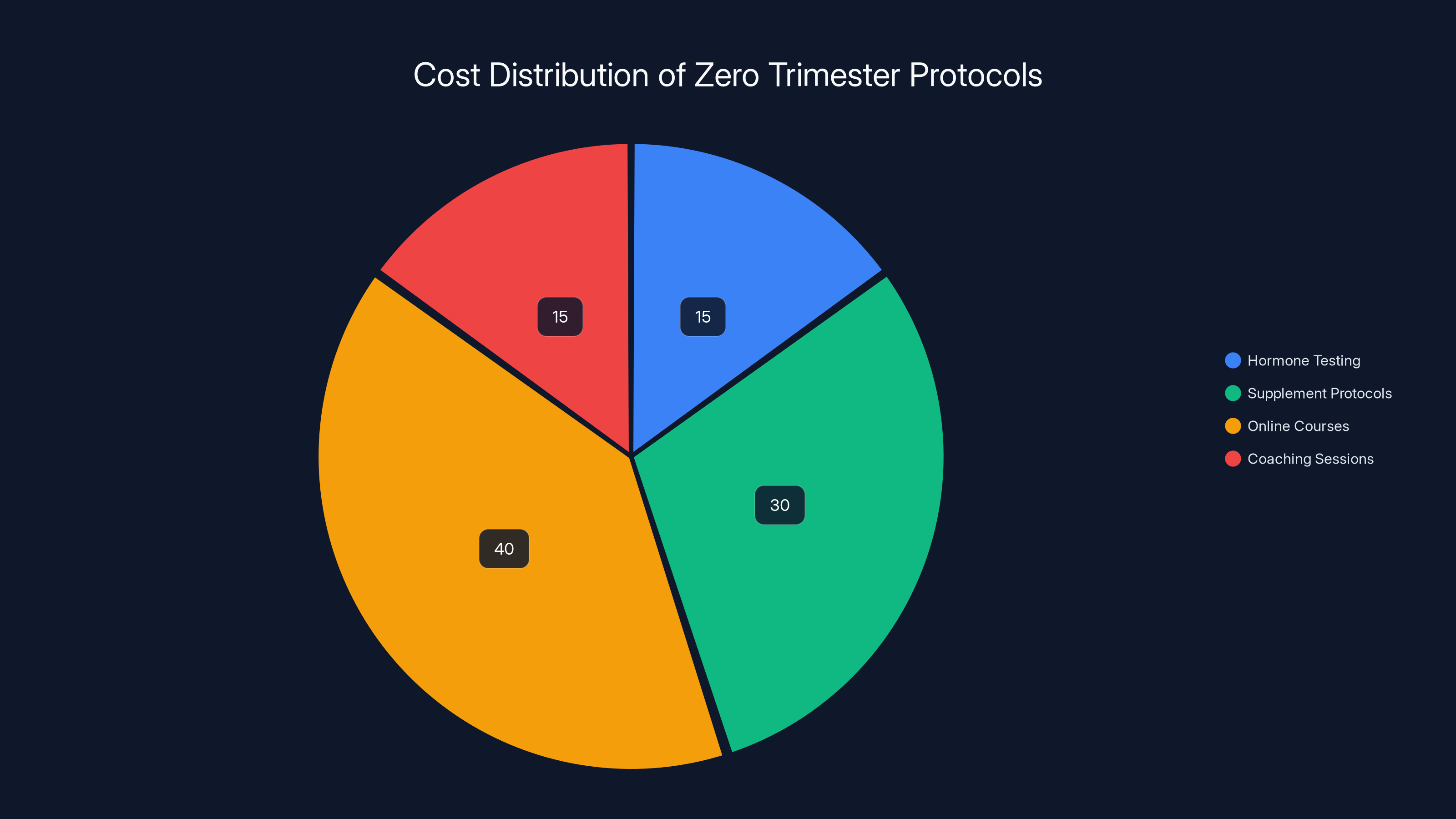
The majority of costs in zero trimester protocols are attributed to online courses and supplement protocols, which together account for 70% of the total estimated annual expense.
The Financial Incentive Structure: Who's Making Money
Follow the money in the zero trimester movement, and the picture becomes clearer. This isn't just wellness philosophy; it's a sophisticated marketing and monetization ecosystem.
At the base level are supplement companies. The preconception supplement market is enormous and largely unregulated. While the FDA oversees drugs, dietary supplements operate with minimal scrutiny. A company can make claims about "supporting reproductive health" or "promoting healthy eggs" without rigorous clinical evidence. When an influencer with 500,000 followers recommends a specific supplement, suddenly thousands of people are buying bottles they didn't know they needed.
Many successful pregnancy prep influencers have launched their own supplement brands. They develop a preconception protocol on social media, build an audience convinced of its necessity, then launch a branded supplement line recommended to followers. The margins on supplements are extraordinary—retail markups of 300-500% are standard. An influencer with even modest conversion rates can generate six-figure monthly revenue.
Then there are the testing services. Companies like Oligo Scan, specialized hormone panels beyond standard medical testing, Dutch hormone testing, micronutrient analyses—these services exist in a regulatory gray area. They're marketed directly to consumers ("DTC" in industry jargon), often through influencer recommendations. A single test might cost
Course platforms represent another layer. Influencers develop online courses—"Optimize Your Fertility in 12 Weeks," "The Complete Preconception Blueprint," "Egg Health Mastery," etc. These courses typically cost
One-on-one coaching creates the highest-margin opportunity. A functional nutritionist or health coach with strong social media presence can charge
The ecosystem also includes wellness retreats, specialized fertility clinics that operate outside mainstream medical frameworks, "functional medicine" practitioners (many of whom aren't traditionally licensed medical doctors), and lifestyle brands selling everything from "fertility-friendly" cookware to menstrual cycle tracking apps to EMF-blocking clothing.
The financial incentives create a version of a Goodhart's Law problem: "When a measure becomes a target, it ceases to be a good measure." When the metric is "engagement" and "follower growth," the content incentives push toward increasingly extreme claims, more elaborate protocols, and constant expansion of the "necessary" interventions. A simple, evidence-based message ("Take prenatal vitamins, exercise, manage stress") doesn't drive engagement. An elaborate biohacking protocol that requires constant optimization, supplementation, testing, and expert guidance—that drives engagement, followers, and revenue.
The Access Problem: Privilege and Fertility Optimization
One of the most troubling aspects of the zero trimester movement is how it's structured around privilege and access. These optimization protocols aren't accessible to most women, yet they're presented as necessary for healthy pregnancy outcomes.
Consider the time investment alone. Researching fertility protocols, shopping for "clean" personal care products, learning about supplement protocols, tracking metrics, attending online courses, booking and attending coaching sessions—this easily requires 10-20+ hours weekly. This is only feasible for women with flexible schedules and discretionary time. Women working multiple jobs, single mothers, women in careers with inflexible schedules, women living in rural areas with limited access to specialized practitioners—they're effectively excluded from these protocols.
The financial barrier is even more stark. We've already outlined costs:
There's also a geographic dimension. Functional medicine practitioners, fertility coaches, and specialized testing services cluster in major urban centers and affluent suburbs. Women in less affluent areas or rural communities may have no access to these practitioners at all, even if they could afford them.
This geographic and class dimension is particularly troubling because it intersects with existing disparities in maternal health. Black women in the United States have maternal mortality rates 2.6-3.5 times higher than white women. These disparities are driven by systemic racism in healthcare, not by insufficiently optimized preconception protocols. Yet the zero trimester movement implicitly suggests that inadequate fertility optimization is a significant factor in pregnancy complications—a narrative that centers individual behavior change rather than systemic healthcare inequities.
The movement also creates a class marker. Just as expensive wellness goods (organic produce, high-end gym memberships, wellness retreats) have become signals of affluence and social status, so has fertility optimization. Women in affluent communities share their preconception protocols with the same aesthetic and status-signaling purpose as they share beach vacation photos. It's a form of conspicuous consumption, except the consumption is framed as health-related rather than frivolous.
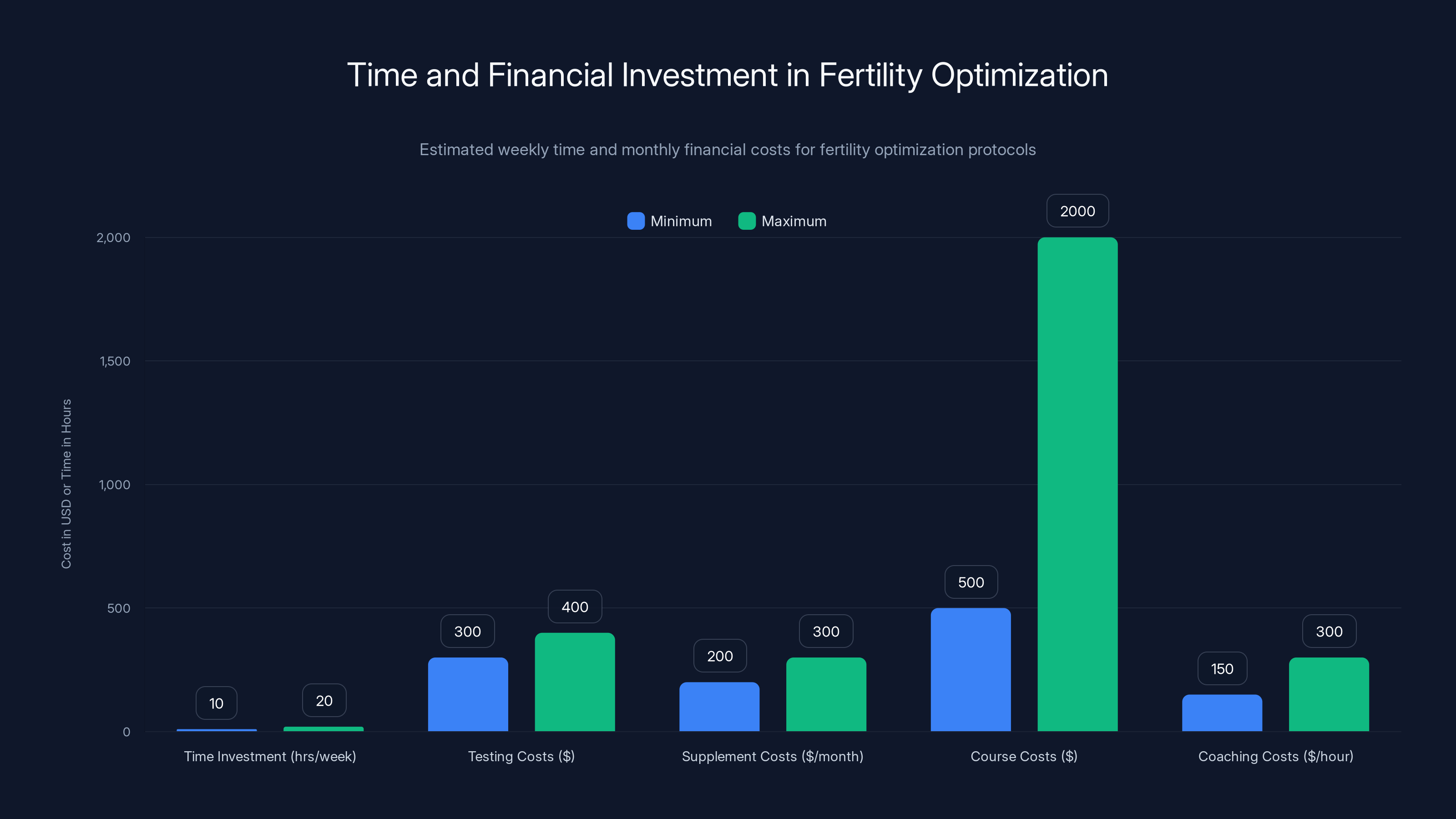
Fertility optimization requires significant time (10-20 hours weekly) and financial investment, making it accessible primarily to affluent women. Estimated data.
The Psychological Toll: Perfectionism, Anxiety, and Responsibility
Beyond the financial and access dimensions, the zero trimester movement exerts a psychological toll that deserves serious attention.
It creates a framework where pregnancy outcomes become entirely an individual woman's responsibility. If you follow the protocol correctly and still struggle to conceive, experience miscarriage, or have pregnancy complications, the implicit message is that you failed. You didn't optimize hard enough. You didn't take enough supplements. You didn't eliminate enough toxins. You didn't manage your stress adequately.
This is psychologically devastating and empirically false. Fertility and pregnancy outcomes are influenced by numerous factors—genetic variation, age, undiagnosed medical conditions, partner factors, and yes, some modifiable lifestyle factors. But they're also influenced by random biological variation that no amount of optimization can control. Approximately 15% of couples will experience difficulty conceiving, and many of these cases involve no identifiable cause. No protocol can change that.
The zero trimester movement also creates a particular form of anticipatory grief. Women are encouraged to mourn a pregnancy that hasn't happened, to feel responsible for a child that doesn't exist, to optimize their bodies for a future that's uncertain. This extends the emotional investment in fertility far backward into time—not just during the months of actively trying to conceive, but during the preceding years of "preparation."
For women with existing anxiety or obsessive-compulsive tendencies, the protocol can become a compulsion. The logic is straightforward: each additional intervention reduces risk, so more interventions are better. A woman might find herself performing increasingly elaborate routines—specific sunrise-viewing protocols, exact supplement timing, elimination of more and more foods or products. The anxiety reduction is temporary. Soon, something else emerges as a potential threat requiring intervention.
There's also a particular form of perfectionism embedded in the zero trimester narrative. It positions pregnancy as a challenge to be "won" through optimization, with the implication that women who achieve "perfect" pregnancies (no complications, easy labor, healthy baby) did so because they optimized correctly. This erases the role of privilege, luck, and random biology. It frames pregnancy as a performance to be mastered rather than a natural biological process with inherent unpredictability.
Cultural Narratives: Choice, Control, and the Myth of Perfect Preparation
The zero trimester movement operates within broader cultural narratives about choice, control, and individual responsibility. Understanding these narratives is crucial to understanding why the movement resonates so powerfully.
The "choice" narrative positions fertility and pregnancy as something women can fully control. This appeals to feminist ideals of autonomy and agency. The implicit pitch is: you don't have to be at the mercy of biology. You can engineer the outcome you want. This sounds empowering. And in some limited ways, it is. Exercise, prenatal vitamins, and stress reduction are things you can control that do affect outcomes.
But the narrative extends far beyond these evidence-based interventions into a realm where control is illusory. You cannot control whether you have a genetic predisposition to miscarriage. You cannot control whether your partner has sperm factor issues. You cannot control whether your ovaries respond well to hormonal stimulation if you require fertility treatments. You cannot control the random biological events that determine whether a conceived embryo implants and develops normally.
The "control" narrative also obscures the role of privilege and luck. A woman with access to excellent prenatal care, no economic stress, a supportive partner, good genetics, and timing luck will have better pregnancy outcomes than an uninsured woman in a healthcare desert working two jobs. The zero trimester narrative suggests the first woman's advantage comes from superior optimization. It doesn't. It comes from privilege.
There's also a narrative of "natural" fertility optimization—the idea that through the right lifestyle practices, women can restore their fertility to some optimal state. This obscures the fact that fertility changes over time (age is the single strongest predictor of fertility potential) and that some fertility challenges are biological rather than behavioral. Marketing supplements to women in their 40s as a path to "natural" conception when their fertility has declined due to age-related factors is misleading at best, cruel at worst.
The marathon training analogy, popular among pregnancy prep influencers ("You'd spend months planning a wedding, why not your pregnancy?"), encodes assumptions worth examining. It assumes that pregnancy is a challenge to be trained for, an event you win or lose based on your preparation. It suggests that pregnancy outcomes correlate primarily with individual effort. It positions the woman's body as terrain to be conquered through discipline and optimization.
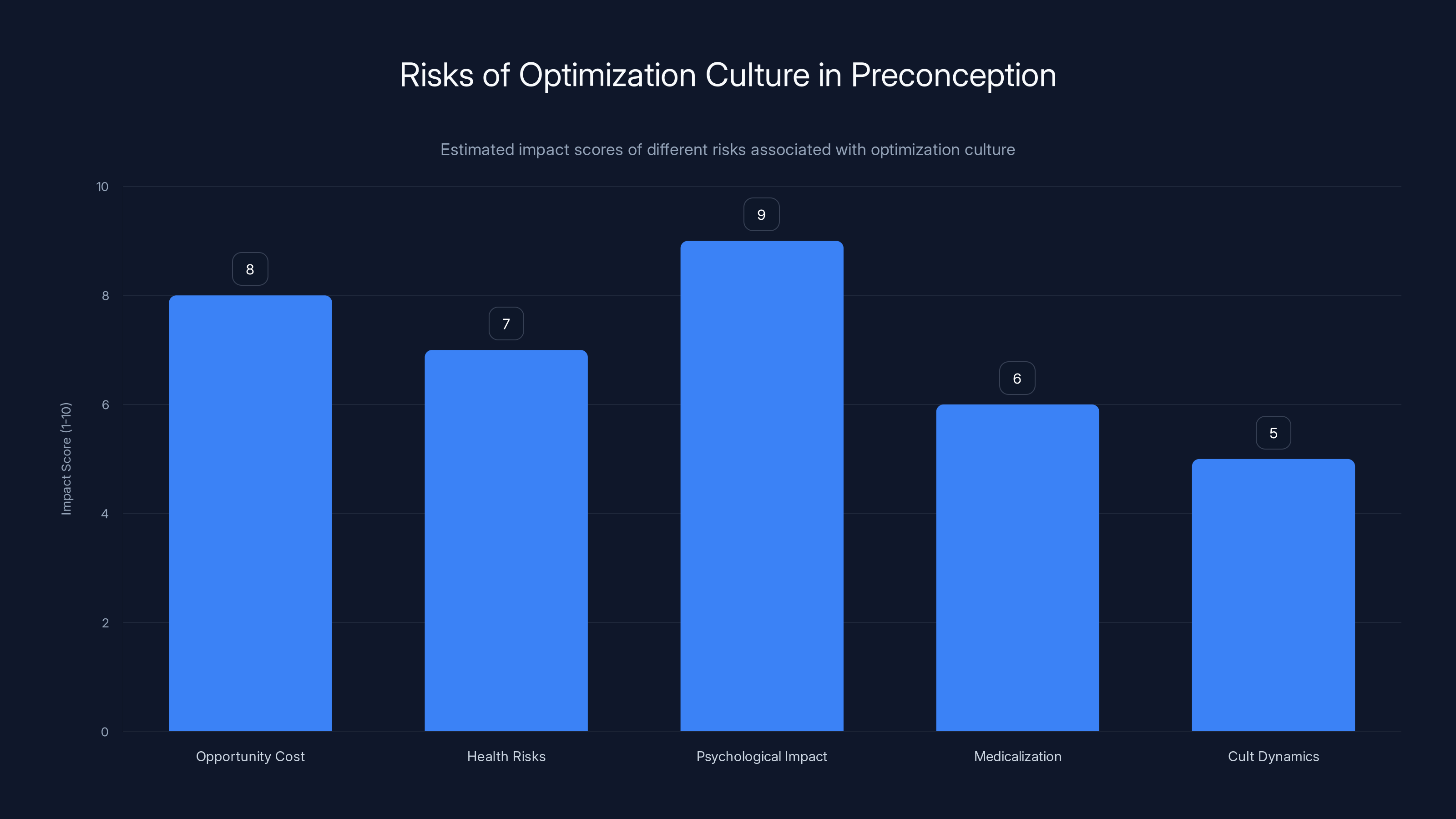
Estimated data shows psychological impact as the highest risk in optimization culture, followed by opportunity cost and health risks.
What Reproductive Endocrinologists Actually Recommend
It's worth pausing here to consider what reproductive medicine specialists—doctors who have extensive training in fertility and pregnancy—actually recommend for preconception health.
The American College of Obstetricians and Gynecologists recommends: prenatal vitamins containing folic acid, health habit optimization (exercise, nutrition, stress management, avoiding substances of abuse), screening for sexually transmitted infections, management of chronic conditions, vaccination updates, and discussion of family history to assess genetic risks. That's it. The guidance hasn't changed substantially in decades because the evidence supporting these interventions is strong and stable.
For women with diagnosed fertility challenges or who haven't conceived after 12 months of attempting (or 6 months if over age 35), reproductive endocrinologists may recommend further testing. But this further testing aims to identify treatable problems—ovulation disorders, sperm factor issues, tubal blockages, endometriosis—not to look for subtle "imbalances" that require months of supplementation to correct.
Most reproductive endocrinologists are skeptical of the zero trimester movement. They see women arriving for fertility evaluations after spending months or years on elaborate optimization protocols, with no improvement in fertility outcomes. They see women's anxiety escalating as the protocols fail to deliver promised results. They see the protocols sometimes interfering with medical care—women reluctant to use necessary medications because they're not "natural," or women delaying appropriate diagnostic workup because they're convinced the problem is environmental toxin exposure rather than medical.
The fundamental disagreement comes down to this: mainstream reproductive medicine views preconception health as important but limited. Certain interventions (prenatal vitamins, avoiding harmful substances, treating medical conditions) matter. But beyond that, there's a recognition that human fertility involves biological variation and that you can't optimize your way around genetic or age-related limitations.
The zero trimester movement, by contrast, suggests that fertility is highly plastic—responsive to environmental, behavioral, and supplemental interventions that go far beyond standard medical recommendations. The reproductive medicine community largely rejects this view because it's not supported by evidence.
The Real Risks of Optimization Culture
While much of the zero trimester movement is simply ineffective (unlikely to harm, just not useful), some aspects carry genuine risks worth considering.
First, there's the opportunity cost. Women spending $5,000 and hundreds of hours on unproven preconception protocols might instead invest that time and money in evidence-based care. If they actually have fertility challenges, this delay can be costly. Fertility declines with age, especially after 35. Months spent trying unproven interventions before seeking medical evaluation can cost valuable time.
Second, some specific interventions carry health risks. Restrictive diets promoted by some zero trimester protocols (ketogenic diets, elimination diets removing multiple food groups) can lead to nutrient deficiencies at a time when adequate nutrition matters. Excessive supplementation can also cause problems. Some supplements interact with medications. Some are poorly regulated and may contain contaminants. High-dose vitamin A supplements, sometimes recommended in fertility protocols, can cause birth defects if pregnancy occurs.
Third, there's the psychological risk of failed optimization. When women follow an elaborate protocol and don't conceive, the psychological impact can be severe. They've internalized the message that pregnancy is a choice they control, so failure to conceive becomes a personal failure. This can lead to depression, anxiety, and crisis of self-worth.
Fourth, there's the medicalization of normal variation. Some zero trimester protocols encourage extensive hormone testing to identify "imbalances." But hormone levels vary naturally throughout the cycle and across individuals. Natural variation gets pathologized—a slightly elevated FSH becomes a problem requiring intervention, when it might be entirely normal. This can lead to unnecessary treatment of non-existent conditions.
Fifth, there's potential for cult dynamics. Women in online zero trimester communities reinforce each other's beliefs, create in-group identity around the protocols, and discourage questioning. When someone expresses doubt about the protocols or suggests following mainstream medical guidance instead, they face social pressure. This can trap women in increasingly elaborate and costly interventions.
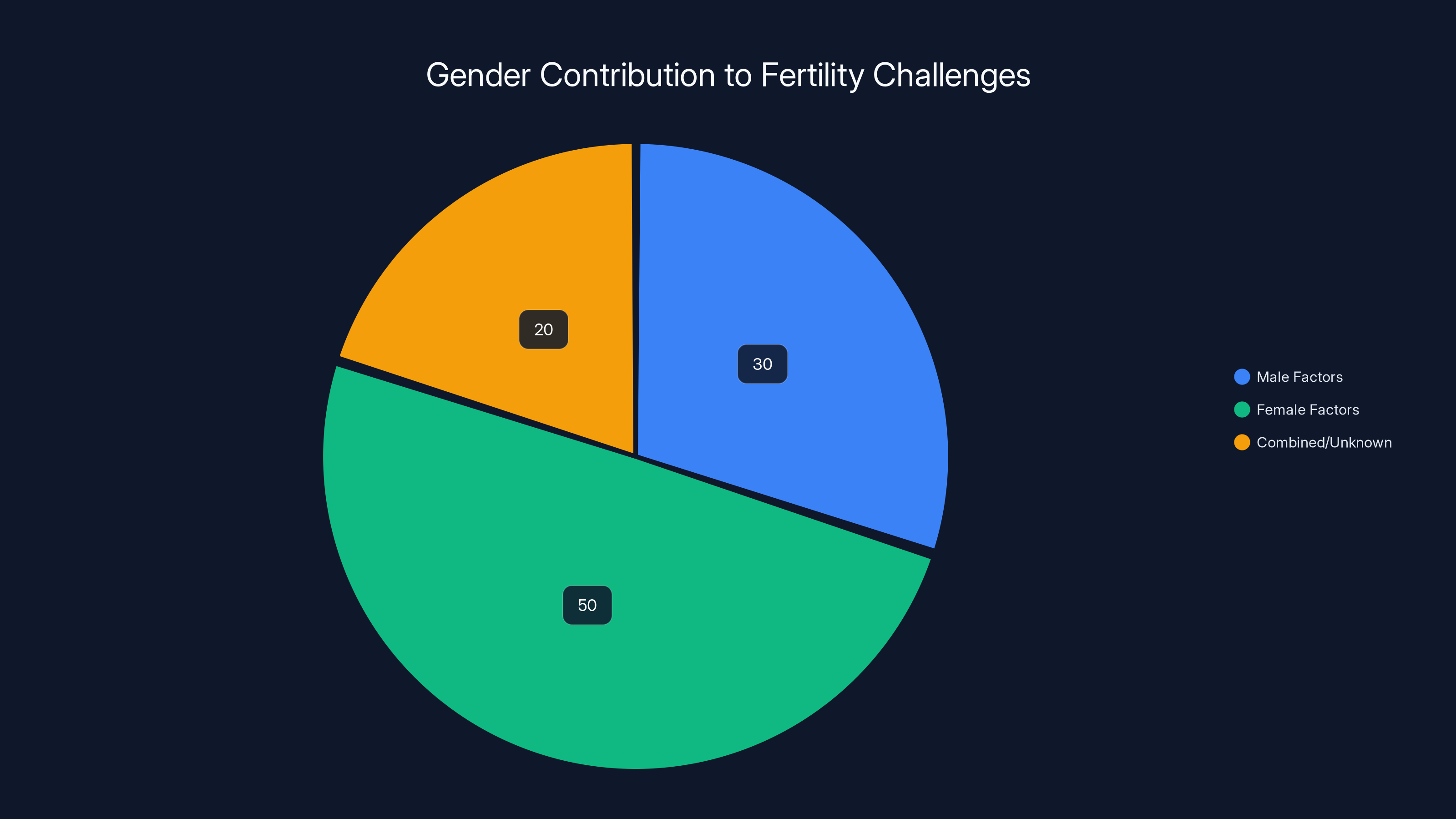
Estimated data shows that male factors contribute to 30% of fertility challenges, highlighting the gendered focus of the zero trimester movement on women.
The Influencer-Doctor Divide: Where Expertise Collides
One of the most interesting tensions in the zero trimester landscape is between traditional medical authority and social media authority. Both claim expertise. Both present solutions. But they often directly contradict each other.
A mainstream OB-GYN might tell a woman: "You're 32, no medical problems, trying to conceive for 3 months. This is normal variation. Keep taking prenatal vitamins, stay generally healthy, and don't stress. Come back if you haven't conceived in a year."
A zero trimester influencer with 500,000 followers, meanwhile, tells the same woman: "Three months is too long to wait. Your egg quality might be declining. You need comprehensive hormone testing, a specialized supplement protocol, possibly dietary modification and stress management coaching. Here's my course on optimizing fertility outcomes."
These messages operate in fundamentally different frameworks. Medicine relies on population-level evidence and statistical significance. An intervention is recommended if it shows meaningful improvement in outcomes in rigorous studies. Influencer advice relies on individual stories and anecdotes. If one follower conceived after following a protocol, that becomes testimonial evidence, regardless of whether she would have conceived anyway.
Medicine also operates on a risk-benefit framework. Prenatal vitamins are recommended because the benefits (reduced birth defects) clearly outweigh costs (minimal risk, low cost). Many zero trimester interventions operate with an assumption of asymmetrical risk: they might help, and the downside is just money and time. But this ignores psychological costs and opportunity costs.
Medianely, there's also a structural difference in how they treat uncertainty. Medicine tends to embrace uncertainty, acknowledging what's unknown. Influencers tend to fill uncertainty with confident assertions. This actually appeals to people—the confident expert who claims to have decoded a puzzle is more engaging than the careful expert who says "we don't know enough to make specific recommendations beyond standard care."
The Gender Dimension: Why This Matters
It's crucial to recognize that this phenomenon is gendered in important ways. The zero trimester movement is primarily directed at women. While male fertility factors contribute to approximately 30% of couples' fertility challenges, there's no parallel movement of men training for paternity or optimizing their reproductive capacity through elaborate supplementation protocols.
This reflects broader patterns in how reproductive responsibility is allocated. Women are culturally assigned primary responsibility for reproductive outcomes—whether pregnancy occurs, whether it goes smoothly, whether the baby is healthy. Men are typically expected to be secondary contributors. In the zero trimester movement, this shows up explicitly: women are told their preconception health is crucial; male partners occasionally get a mention but rarely the intensive focus.
There's also a gendered dimension to who's profiting from this movement. While some of the most prominent zero trimester influencers are women, they're typically marketing expertise (usually self-proclaimed, sometimes with legitimate credentials) to women. They're extracting value from other women's anxiety and desire to be "good mothers" before motherhood even begins.
The movement also reflects a particular type of feminine perfectionism—the assumption that women should be constantly optimizing, constantly improving, constantly taking responsibility for outcomes that are partially outside their control. It's the feminine version of the biohacking impulse that drives men to track metrics, engineer their bodies, and optimize productivity. Except for women, it's specifically about reproductive capacity and the promise of perfect children.
This creates a particular form of reproductive labor—not the physical labor of pregnancy and childbirth, but the emotional and temporal labor of constant fertility optimization. It's unpaid, often invisible work that women are encouraged to take on before they're even pregnant.
When Preconception Health Makes Sense: Evidence-Based Recommendations
Amid all this criticism, it's important to emphasize: preconception health matters. The problem isn't the concept; it's the execution and the monetization.
Here's what actually matters before pregnancy: Take a prenatal vitamin with at least 400 micrograms of folic acid daily. If you have a history of neural tube defect pregnancy, take 4 milligrams daily. Maintain a healthy weight—not through crash dieting, but through sustainable habits that would benefit you whether or not pregnancy was planned. Exercise regularly, aiming for 150 minutes of moderate-intensity activity weekly. Eat a reasonably balanced diet with adequate protein and micronutrients. Avoid smoking, heavy alcohol use, and illicit drugs. Manage chronic conditions like diabetes, hypertension, or depression. Get vaccinated if you're not immune to rubella. Screen for sexually transmitted infections. Take folic acid supplementation for the 3-6 months before attempting pregnancy (or just continuously once you're in the age range where pregnancy is possible).
Do all this, and you've done 95% of what evidence suggests matters for preconception health. You don't need organic berries. You don't need specialized hormone testing. You don't need pelvic floor Pilates. You don't need to eliminate LED lights or sleep with your phone in another room. You don't need to spend thousands of dollars.
If after a year of attempting pregnancy (or 6 months if you're over 35), you haven't conceived, then seek medical evaluation. If you have known risk factors for fertility challenges (irregular periods, previous ectopic pregnancy, endometriosis, partner with known fertility issues), consider earlier evaluation. Medical evaluation can identify treatable problems—ovulation disorders, tubal blockages, sperm factor issues—that explain why conception hasn't occurred and that can be addressed with appropriate medical care.
But for the vast majority of women, the pathway to pregnancy is: basic health practices, prenatal vitamins, and patience. Not elaborate optimization protocols, specialized testing, or expensive courses.

Future Directions: Will This Trend Persist or Fade?
Will the zero trimester movement continue to grow, or is it a transient cultural moment?
Several factors suggest it will likely persist and potentially expand. The economic incentives are substantial and growing. As the fertility supplement market expands, more companies will invest in influencer partnerships and social media marketing. As social media algorithms reward engagement (and fertility optimization content drives engagement through fear and aspiration), platforms will continue surfacing this content to relevant audiences.
The cultural conditions that enable this movement also show no signs of changing. Women continue to face tremendous pressure to be perfect mothers before and during pregnancy. The perception that parenting requires constant optimization remains strong. Economic inequality continues to grow, creating pressure among affluent women to purchase status-signaling goods (including fertility optimization protocols). Climate anxiety and environmental health concerns (real and exaggerated) drive interest in detoxification and environmental control narratives.
However, there are countervailing forces. As more women go through elaborate zero trimester protocols and don't experience the promised outcomes, some will become skeptical. As more reproductive endocrinologists publicly criticize the movement, some credibility will transfer from influencers to medical professionals. If regulatory agencies begin scrutinizing the marketing claims made by fertility supplement companies or functional medicine practitioners, some of the infrastructure supporting this movement may face legal challenges.
There's also potential for the zero trimester movement to evolve. As more evidence emerges about effective preconception interventions, influencers could pivot toward more evidence-based messaging. Some already market "science-backed" fertility protocols—which is more honest than claiming expertise they lack, even if some of those protocols still stretch evidence beyond what it supports.
The most likely scenario is that the movement persists and possibly expands among affluent, highly-educated women (the demographic most engaged with wellness culture and most able to afford these protocols) while having less influence on women with fewer resources. This would deepen existing inequalities in reproductive care and outcomes.
Navigating Preconception Health in a Confused Landscape
For women trying to navigate preconception health decisions in an increasingly confusing landscape, here are some useful principles.
First, distinguish between evidence-based interventions and interventions promoted primarily through social media. Check whether major medical organizations endorse specific recommendations. If ACOG, ASRM (American Society of Reproductive Medicine), or CDC guidelines mention something, it's more likely to have substantial evidence. If you're reading about it primarily on Instagram, be skeptical.
Second, be suspicious of confidence. The more certain an expert sounds about subtle biological mechanisms, the more uncertain you should become. Real experts acknowledge limitations and acknowledge what's not known. Influencers tend to be maximally confident, even when discussing subjects where scientific confidence is low.
Third, follow the money. If someone is selling products or services related to fertility optimization, they have financial incentive to convince you that optimization is necessary. This doesn't mean their advice is wrong, but it's a reason to view it with appropriate skepticism.
Fourth, remember that fertility is probabilistic, not deterministic. Even optimally healthy women don't have 100% conception rates. Some couples take months or years to conceive despite doing everything "right." This is normal biological variation, not evidence of inadequate optimization.
Fifth, don't delay medical care. If you have concerns about fertility or if you haven't conceived after a year of attempting (or 6 months if over 35), seek medical evaluation. Early identification of treatable fertility problems genuinely matters. Waiting while trying unproven optimization protocols can waste valuable time.
Sixth, beware of perfectionism. You don't need a perfect preconception protocol. You don't need to eliminate every potential toxin or optimize every biological parameter. A healthy pregnancy after minimal preconception optimization is normal and common. A healthy pregnancy outcomes doesn't require an elaborate protocol.

What We Still Don't Know: Research Gaps and Uncertainty
For all the confidence zero trimester influencers express about fertility mechanisms and optimization strategies, there's actually substantial scientific uncertainty about many aspects of reproductive health. Understanding what we don't know is important for interpreting claims.
We don't fully understand individual variation in egg quality or what actually determines whether an embryo implants and develops normally. We have crude measures (egg count via ultrasound, age-based decline in fertility) but no reliable test for individual egg quality short of fertilizing and growing embryos. Many marketed products claim to improve "egg quality," but we lack reliable biomarkers to measure whether they actually do.
We don't fully understand the mechanisms by which body weight affects fertility or what the optimal "target" weight is for conception. We know that extreme obesity and extreme leanness both reduce fertility, but the biological mechanisms aren't entirely clear, and the optimal range varies between individuals.
We don't fully understand how environmental exposures at levels currently encountered in developed countries affect fertility. We know some exposures (like high-dose pesticide exposure) reduce fertility. We don't know whether the levels of phthalates, BPA, or other endocrine-disrupting chemicals that people encounter through normal consumer products meaningfully impair fertility.
We don't have good evidence for most specialized supplementation protocols aimed at improving fertility. We have evidence that general health (adequate nutrition, appropriate weight, exercise) matters. We don't have high-quality trials showing that specific supplement combinations improve fertility in women without known deficiencies.
We don't understand all the reasons why some couples struggle to conceive. In up to 15-25% of couples, no cause is identified despite extensive medical workup. The zero trimester movement often implicitly suggests these are behavioral/environmental cases where optimization would help—but that's not necessarily true.
These knowledge gaps are exactly why the zero trimester movement finds fertile ground (pun intended). When science is uncertain, narratives can flourish. When the mechanisms aren't entirely clear, plausible-sounding stories can gain traction. The responsible response to this uncertainty would be humility—acknowledgment of what we don't know. Instead, influencers fill the uncertainty with confident assertions, and followers, desperate for control and guidance, embrace the certainty even when the actual evidence is thin.
The Bottom Line: Questioning Assumptions About Pregnancy Preparation
The zero trimester movement represents something deeper than just wellness trend or influencer marketing (though it's certainly both). It represents a fundamental assumption about control, responsibility, and the nature of human biology.
The assumption is that pregnancy is a project to be managed, optimized, and controlled through sufficiently informed and disciplined effort. The corollary assumption is that if something goes wrong—if you struggle to conceive, if pregnancy is complicated, if your baby has health issues—it's at least partially your fault for not optimizing thoroughly enough.
But this assumption clashes with biological reality. Human reproduction involves genetic variation, age-related changes, random developmental events, and yes, some environmental and behavioral factors. You have some influence over that last category. You don't have much influence over the others. The idea that you can optimize your way into a perfect pregnancy if you just follow the right protocol is appealing but largely illusory.
This doesn't mean preconception health is irrelevant. It means it's one input among many, and it's less influential than the zero trimester movement suggests. A woman who takes prenatal vitamins and otherwise maintains reasonable health will have similar pregnancy outcomes to a woman who spends $5,000 on specialized testing and supplements. The difference in outcomes comes from genetics, luck, age, and medical factors—not from the marginal effect of elaborate optimization.
The movement will likely persist because it serves real psychological and economic needs. People want to believe they control outcomes. Companies profit from selling that belief. Influencers build audiences and income by promoting it. But from a public health perspective, the movement is probably doing more harm than good—creating anxiety, wasting resources, deepening health inequities, and promoting a distorted view of how reproduction works.
The healthiest approach to preconception planning is probably boring: take prenatal vitamins, maintain general health practices you'd want anyway, avoid clearly harmful substances, and let biology proceed. If conception doesn't happen naturally after a reasonable period, seek medical care. If it does happen, proceed with confident humility—knowing that you did what you reasonably could and that much of what happens next is beyond your control.
That's not as exciting as a 12-week preconception optimization program. It doesn't generate engagement on social media. It doesn't sell supplements. But it's grounded in evidence and realistic about what human beings can actually control. And maybe that's worth something.

FAQ
What exactly is the "zero trimester" and why is it becoming so popular?
The zero trimester refers to the period before pregnancy, coined by sociologist Miranda Waggoner to describe when women make lifestyle and health decisions that may influence conception and pregnancy outcomes. It's becoming popular due to social media influence, the broader cultural obsession with optimization, and women's legitimate desire to do everything possible for a healthy pregnancy—combined with effective marketing from wellness influencers promoting specialized supplements and protocols.
Is there scientific evidence that elaborate preconception protocols improve fertility or pregnancy outcomes?
Limited evidence supports most elaborate zero trimester protocols beyond standard medical recommendations. While evidence-based preconception health (prenatal vitamins with folic acid, maintaining healthy weight, managing stress, avoiding harmful substances) does improve outcomes, most specialized interventions promoted by influencers—specialized supplements, hormone testing protocols, detoxification regimens—lack rigorous clinical validation. A 2022 meta-analysis found that for women without diagnosed fertility issues, most preconception optimization doesn't meaningfully affect conception timing or pregnancy outcomes.
How much does following a zero trimester protocol typically cost?
Costs vary widely but can easily exceed
What do reproductive endocrinologists think about the zero trimester movement?
Most reproductive endocrinologists are skeptical of elaborate zero trimester protocols, viewing them as often ineffective and occasionally harmful. They see patients arriving after months or years of optimization without improvement in fertility, escalated anxiety from failed protocols, and sometimes delayed appropriate medical diagnosis. Mainstream reproductive medicine emphasizes that while preconception health matters, most optimization claims exceed what evidence supports.
If I'm trying to conceive, what's the evidence-based approach to preconception health?
Evidence-based preconception care includes taking prenatal vitamins containing at least 400 micrograms of folic acid, maintaining a healthy BMI through sustainable lifestyle practices, exercising 150 minutes weekly of moderate-intensity activity, eating a balanced diet, avoiding smoking and heavy alcohol use, managing chronic conditions, getting appropriate vaccinations, and screening for sexually transmitted infections. Beyond these basics, most additional interventions lack strong evidence supporting meaningful improvement in outcomes.
How can I tell if fertility advice on social media is reliable or exploitative?
Evaluate fertility information by checking whether major medical organizations (ACOG, ASRM) recommend it; being skeptical of maximum confidence when discussing topics where scientific certainty is low; considering whether the person promoting it profits from its adoption; distinguishing between anecdotal individual success stories and population-level clinical evidence; and recognizing that genuinely helpful preconception advice tends to be simple and inexpensive rather than elaborate and costly.
Is it normal to struggle to conceive even while following good preconception health practices?
Yes, completely normal. Approximately 15% of couples struggle with infertility, and this occurs across all health and optimization levels. Approximately 6-12 months of attempting pregnancy is normal before conceiving for women in their prime reproductive years. Genetic variation, age, undiagnosed medical conditions, partner factors, and random biological variation all influence fertility outcomes alongside behavioral factors. Struggling to conceive doesn't indicate you failed at preconception optimization.
Are there any risks to elaborate preconception protocols?
Potential risks include opportunity costs (time and money spent on unproven interventions rather than evidence-based care), nutritional issues from restrictive diets, adverse effects from excessive supplementation, delay in seeking medical evaluation if fertility challenges exist, psychological harm from failed optimization protocols, and reinforcement of anxious perfectionism about pregnancy. For women with existing anxiety or OCD, the protocols can become compulsive and anxiety-reinforcing.
How does the zero trimester movement affect women with fertility problems?
For women with diagnosed fertility challenges, the movement can delay appropriate medical treatment if they spend months on unproven optimization protocols first. It can also create shame and self-blame—the implicit suggestion that infertility results from inadequate preconception optimization rather than medical conditions requiring treatment. Ironically, women with actual fertility problems could often benefit more from timely medical care than from elaborate wellness protocols.
Will this trend fade or is it here to stay?
The zero trimester movement will likely persist and potentially expand due to strong economic incentives for supplement companies and influencers, the psychological appeal of believing you control fertility outcomes, and continued cultural pressure on women to optimize every aspect of reproduction. However, as more women experience failed optimization and as medical professionals continue criticizing the movement, some skepticism may grow. The trend will probably remain strongest among affluent, highly-educated women while having less impact on populations with fewer resources to devote to these protocols.
Conclusion: Reclaiming Realistic Expectations About Pregnancy Preparation
Women planning pregnancy deserve better guidance than what the zero trimester movement currently offers. They deserve evidence-based information delivered without financial incentives to exaggerate intervention importance. They deserve clear communication about what actually matters for preconception health versus what's marketing. They deserve permission to stop optimizing and start living.
The scientific reality is that human reproduction is remarkably robust. Most women conceive without elaborate preparation. Most pregnancies proceed without complications. Most babies are born healthy. These outcomes occur across all optimization levels and across every socioeconomic status. Yes, certain interventions improve the margins. Take prenatal vitamins. Maintain reasonable health. Avoid clearly harmful substances. But beyond that, the gains from additional optimization are typically small.
Moreover, the psychological and financial costs of the zero trimester movement merit serious consideration. Women are being convinced they must spend thousands of dollars and hundreds of hours to be adequate mothers before motherhood begins. They're being told that fertility is a choice completely within their control, setting them up for shame and self-blame if conception doesn't occur on schedule. They're being sold elaborate protocols promising control they ultimately don't have.
A healthier approach would emphasize what evidence actually supports, acknowledge what remains uncertain, and provide permission for women to maintain basic health practices without excessive optimization. It would recognize that perfect pregnancy planning doesn't guarantee perfect outcomes—and that's okay. It would redistribute responsibility away from individual women and toward systemic factors like ensuring all women have access to excellent healthcare regardless of income.
The zero trimester movement likely won't disappear—the economic incentives are too strong and the psychological appeals too powerful. But individual women can choose not to participate. They can recognize that they don't need to train for pregnancy like it's a marathon. They can take prenatal vitamins, maintain reasonable health practices, and proceed with the confident knowledge that they're doing what evidence actually supports. They can resist the narrative that their future child's health depends on their preconception optimization efforts. They can reclaim pregnancy from the optimization culture that's co-opted it and remember that humans have been successfully reproducing for millennia without taking supplements marketed through Instagram or attending paid courses on egg quality.
Pregnancy preparation matters, but less because of what you buy and more because of what you do naturally: eating reasonably, moving your body, managing stress, maintaining relationships, and living a life you find meaningful. Do those things, take your vitamins, and let the rest unfold.
Quick Navigation
- The Zero Trimester Movement
- Understanding the Concept
- The Influencers Building the Empire
- What Science Actually Says
- Financial Incentive Structure
- The Access Problem
- Psychological Toll
- Cultural Narratives
- What Doctors Actually Recommend
- Real Risks of Optimization
- The Influencer-Doctor Divide
- Gender Dimension
- Evidence-Based Recommendations
- Future Directions
- Navigating the Landscape
- Research Gaps
Key Takeaways
- The zero trimester movement represents a $2+ billion industry selling elaborate preconception optimization protocols largely driven by social media influencers rather than medical evidence
- Evidence-based preconception health (prenatal vitamins with folic acid, exercise, healthy weight, stress management) is effective, but most specialized protocols promoted by influencers lack rigorous clinical validation
- The movement creates significant financial barriers and disparities, making fertility optimization accessible primarily to affluent women while implicitly pathologizing natural variation
- Psychological costs include increased anxiety, perfectionism, and false sense of control over inherently unpredictable biological processes
- Reproductive endocrinologists largely reject the elaborate zero trimester protocols as ineffective and sometimes harmful, emphasizing that basic health practices suffice for most women

