![DMT as Antidepressant: Breakthrough Clinical Trial Results [2025]](https://tryrunable.com/blog/dmt-as-antidepressant-breakthrough-clinical-trial-results-20/image-1-1771418340525.jpg)
DMT as a Rapid-Acting Antidepressant: What the Latest Clinical Trial Reveals
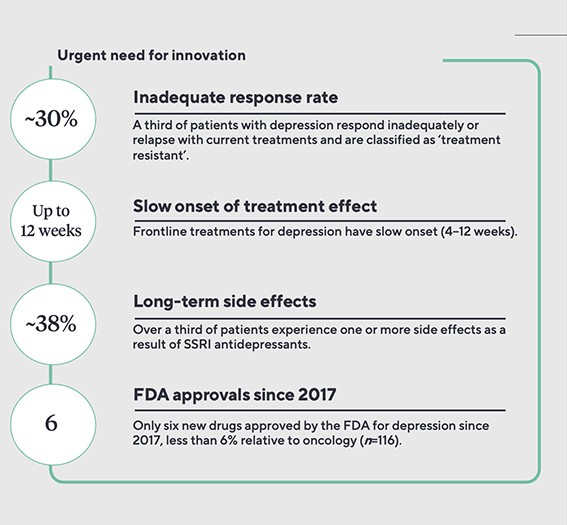
Depression has a way of settling into your life like an unwanted houseguest. It doesn't announce itself loudly—it just quietly rewires how you see the world, making everything feel heavier, slower, more pointless. For decades, the standard response was selective serotonin reuptake inhibitors (SSRIs), which work. Sometimes. For some people. But they can take weeks to kick in, and roughly a third of patients see minimal benefit no matter what dose they take.
Then something unexpected happened. Scientists started looking at psychedelic drugs—substances most people encounter only as cautionary tales or party stories—and found something remarkable: they seemed to offer depression relief in days rather than weeks, and in some cases, the effects stuck around for months.
The latest evidence comes from a small but carefully controlled clinical trial published in 2026 showing that DMT (dimethyltryptamine), the shortest-acting psychedelic known, might be just as effective as psilocybin or LSD at treating depression. This matters because DMT clears your system in minutes, not hours. You take it, your brain gets reconfigured, and you're essentially back to baseline consciousness by dinner.
Here's what the research actually shows, why it's significant, and what it means if you or someone you know is struggling with depression that won't respond to conventional treatment.
Understanding DMT: What It Is and How It Works in the Brain
DMT is a naturally occurring compound found in small quantities in the human brain, some animals, and various plants. Chemically, it's a tryptamine—part of the same family that includes serotonin, the neurotransmitter that SSRIs try to boost. But DMT's relationship to depression is far more complex than simply increasing serotonin levels.
In its pure form, DMT is a white crystalline powder that's nearly impossible to dose with precision. This is why traditional use involves ayahuasca, a plant brew that combines DMT-containing plants with others that inhibit monoamine oxidase (MAO), an enzyme your liver uses to break down DMT. Without this chemical inhibitor, your body metabolizes DMT almost instantly—it has a half-life of about five minutes. This rapid clearance was long considered a disadvantage. How could something that disappears so quickly produce lasting changes in mood and perception?
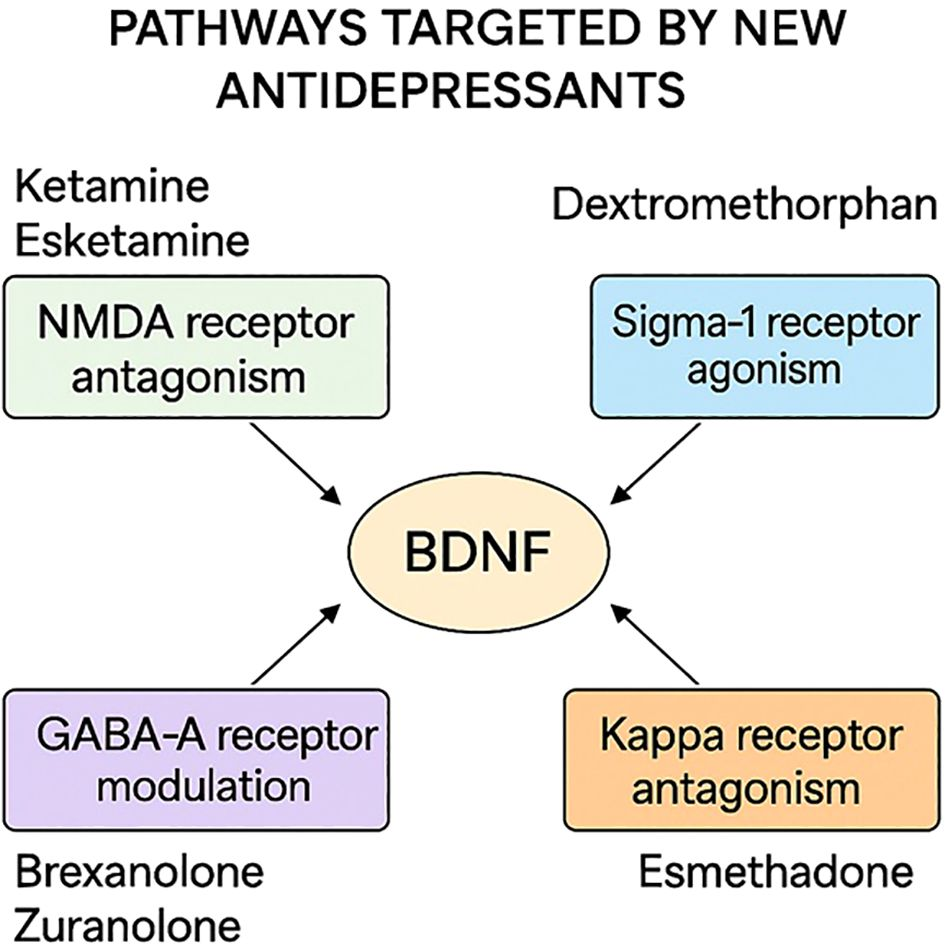
The answer lies in neurotransmitter systems that psychedelics activate, particularly serotonin 2A receptors. These receptors exist throughout the cortex, and when activated, they trigger a cascade of events. The brain increases something called brain-derived neurotrophic factor (BDNF), a protein that essentially tells your neurons to grow new connections. It's like your brain suddenly decides that its current wiring is outdated and needs renovation.
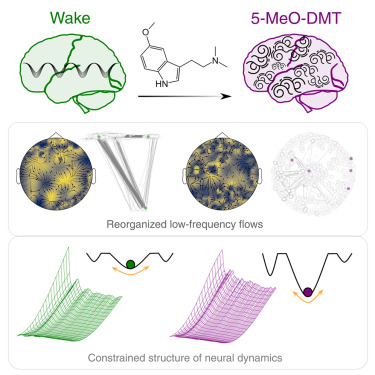
More importantly, these drugs seem to increase neuroplasticity during and after the experience. Neuroplasticity is your brain's ability to rewire itself based on new information and experiences. Depression creates rigid thought patterns—the brain gets stuck in loops that reinforce hopelessness. Psychedelics appear to break these loops by forcing the brain to process information in completely novel ways, then leaving behind more flexible neural architecture.
Researchers at UC San Francisco studying psilocybin found that the drug increases the diversity of neural firing patterns in the days following a dose. Essentially, the brain becomes less predictable, less locked into patterns. This increased flexibility appears to last weeks or months after the drug wears off, even though the acute effects fade in hours.
DMT seems to work through these same mechanisms, but its rapid pharmacokinetics—the speed at which it enters and leaves your system—make it uniquely practical for clinical use. You're not incapacitated for eight hours. You're not anxious about unpredictable effects extending into the next day. This changes everything about how you'd actually implement such a treatment in a real healthcare setting.
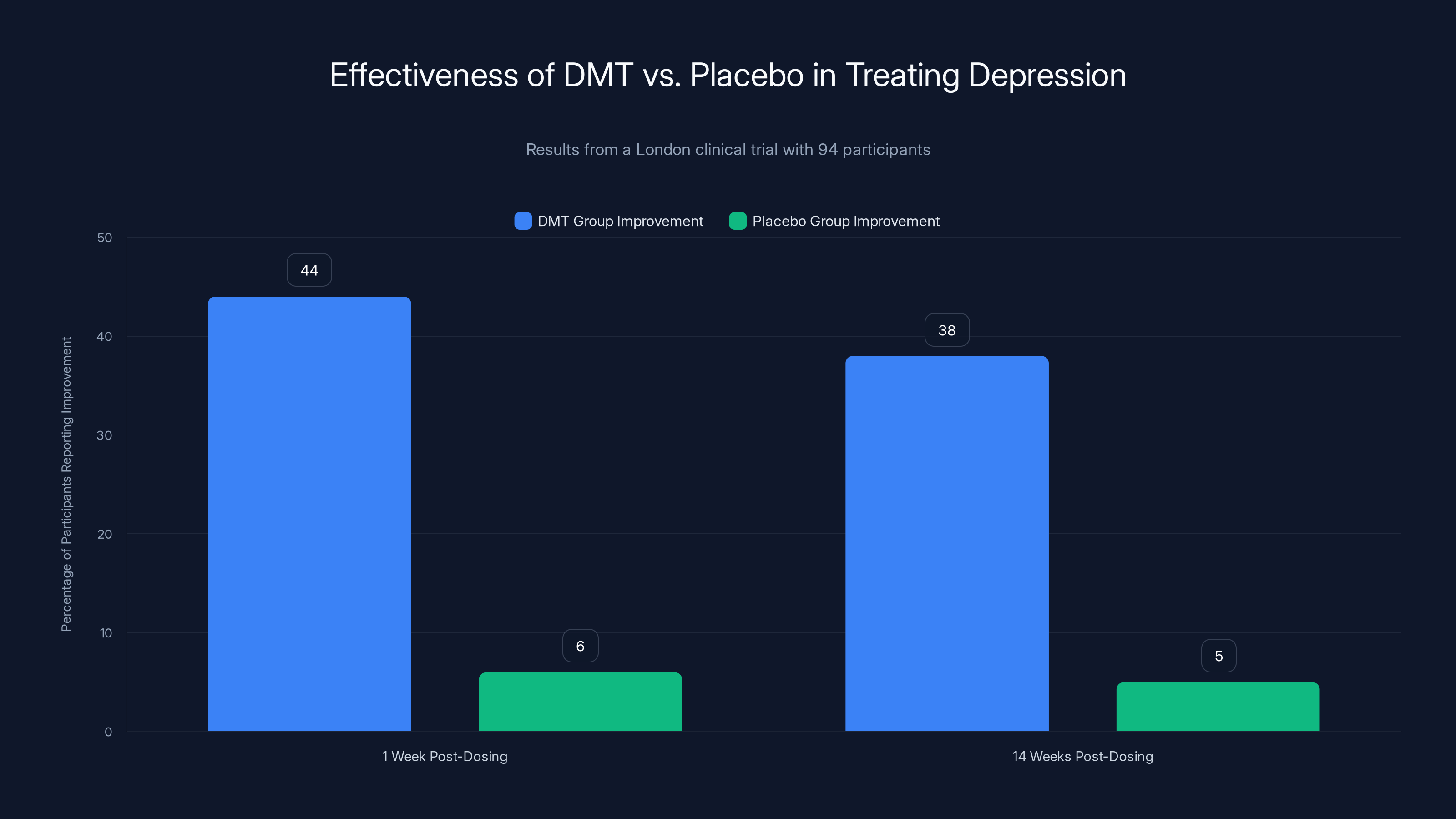
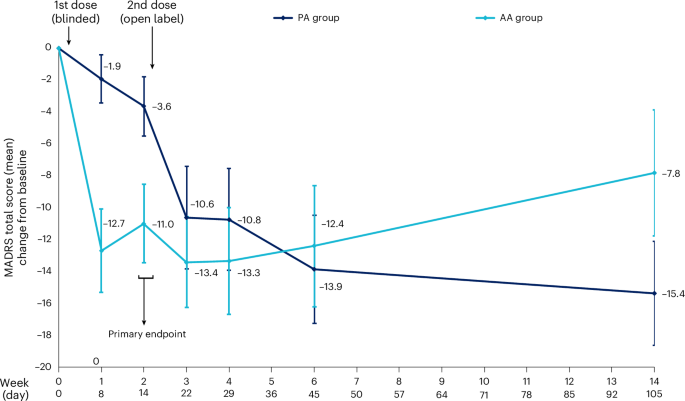
The London clinical trial showed that 44% of participants reported improvement in depression symptoms one week after DMT dosing, with effects largely maintained at 14 weeks. In contrast, the placebo group showed minimal improvement.
The London Trial: First Rigorous Evidence That DMT Works
When researchers from Imperial College London and other institutions designed their DMT trial, they faced a significant challenge: how do you run a blinded trial with a drug that produces intense hallucinations? If you give someone DMT versus a placebo injection, they'll immediately know which one they got because one makes you feel like the universe is made of crystalline geometry and the other doesn't.
The researchers didn't pretend this problem didn't exist. They ran a rigorous design anyway, acknowledging the limitation. The study involved 94 participants with treatment-resistant depression—people who hadn't responded adequately to conventional antidepressants. Participants were split into two groups: one receiving DMT, one receiving placebo saline. Everyone also received structured counseling for depression.
The DMT dose was 20 milligrams, administered as an intravenous infusion over about two minutes. This was chosen to be high enough to produce the intended neurological effects while remaining safely below doses that might cause medical complications.
One week after the initial dose, the differences were stark. Only 6% of the placebo group reported meaningful improvement in depression symptoms. In the DMT group, 44% reported improvement. That's a massive gap—roughly seven times more people feeling better in the psychedelic group compared to controls.
What happened over the following 14 weeks tells an interesting story about how these drugs actually work. The improvements didn't erode back to baseline. Fourteen weeks out, the DMT group remained substantially better. The placebo group also improved over this period, but more gradually—they only received their DMT dose two weeks into the study and showed the same dramatic shift afterward.
This matters because it controls for several confounding variables. The simple act of enrolling in a depression study, receiving medical attention, and having a doctor take your symptoms seriously has real therapeutic value. The placebo group experienced this benefit. But the DMT group experienced something beyond that—the drug itself was doing something.
Side effects were minimal and transient. Participants reported brief spikes in heart rate and blood pressure, which returned to normal quickly. Some had minor pain at the injection site. Importantly, no one experienced the kind of lingering psychological complications that sometimes follow intense psychedelic experiences.
The Mystical Experience Connection: When Spiritual Matters to Your Neurotransmitters
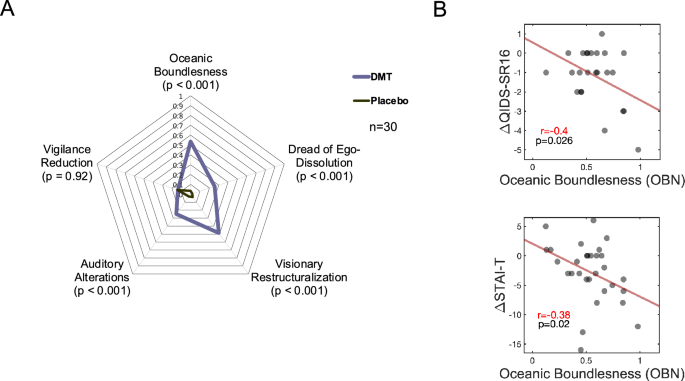
One of the most fascinating findings in the London trial relates to something that initially seems deeply unscientific: whether participants reported a mystical experience. The researchers used the Mystical Experience Questionnaire (MEQ), a standardized assessment that measures the intensity of spiritual or transcendent experiences during psychedelic use.
Participants who reported stronger mystical experiences showed greater antidepressant effects. Those who felt more ego dissolution—essentially, the temporary dissolution of the sense of a separate self—also showed better outcomes. This suggests something counterintuitive: the therapeutic benefit isn't separable from the hallucinogenic experience itself.
This contradicts what some researchers hoped to find. Many drug developers would prefer if they could extract the psychiatric benefits of psychedelics while leaving behind the hallucinations. It's easier to get regulatory approval for a drug that makes you feel better without making you see colors in your peripheral vision that don't exist. It's also less risky and more publicly palatable.
But the data suggests the psychedelic experience is central to the benefit. Why would that be? Several theories exist. The first is that the hallucinations and ego dissolution force psychological processing that wouldn't otherwise occur. Depression involves avoidance—you avoid thinking about certain topics, avoid engaging with parts of yourself, avoid processing certain memories. When your brain chemistry is scrambled and you're experiencing something genuinely novel, you can't avoid. You're forced to engage with the raw experience.
The second theory involves what's called "meaning-making." Humans are meaning-making creatures. We're uncomfortable with random experiences, so we integrate them into our self-narrative. A profound mystical experience during psychedelic use becomes an anchor point—a reference frame for reassessing your life, your depression, your relationship to suffering. Many participants report that the intensity of the experience creates a kind of perspective shift that persists long after the drug wears off.
The third, more biological explanation involves something called "critical period plasticity." Under normal circumstances, your brain's capacity to fundamentally rewire itself decreases after early childhood. Certain drugs can reopen these windows of heightened plasticity. During this window, new learning and experiences get integrated differently—more powerfully. A spiritual or transcendent experience during this window might create neurological changes that persist because they're being written into the brain during a period of heightened malleability.
What's particularly interesting is that the trial didn't separate the drug from the psychological setting. Everyone received counseling. Everyone had professional support. The mystical experience didn't occur in isolation—it occurred within a therapeutic relationship. This suggests that psychedelics might work best not as a replacement for therapy but as an accelerant or catalyst that makes therapy more effective.
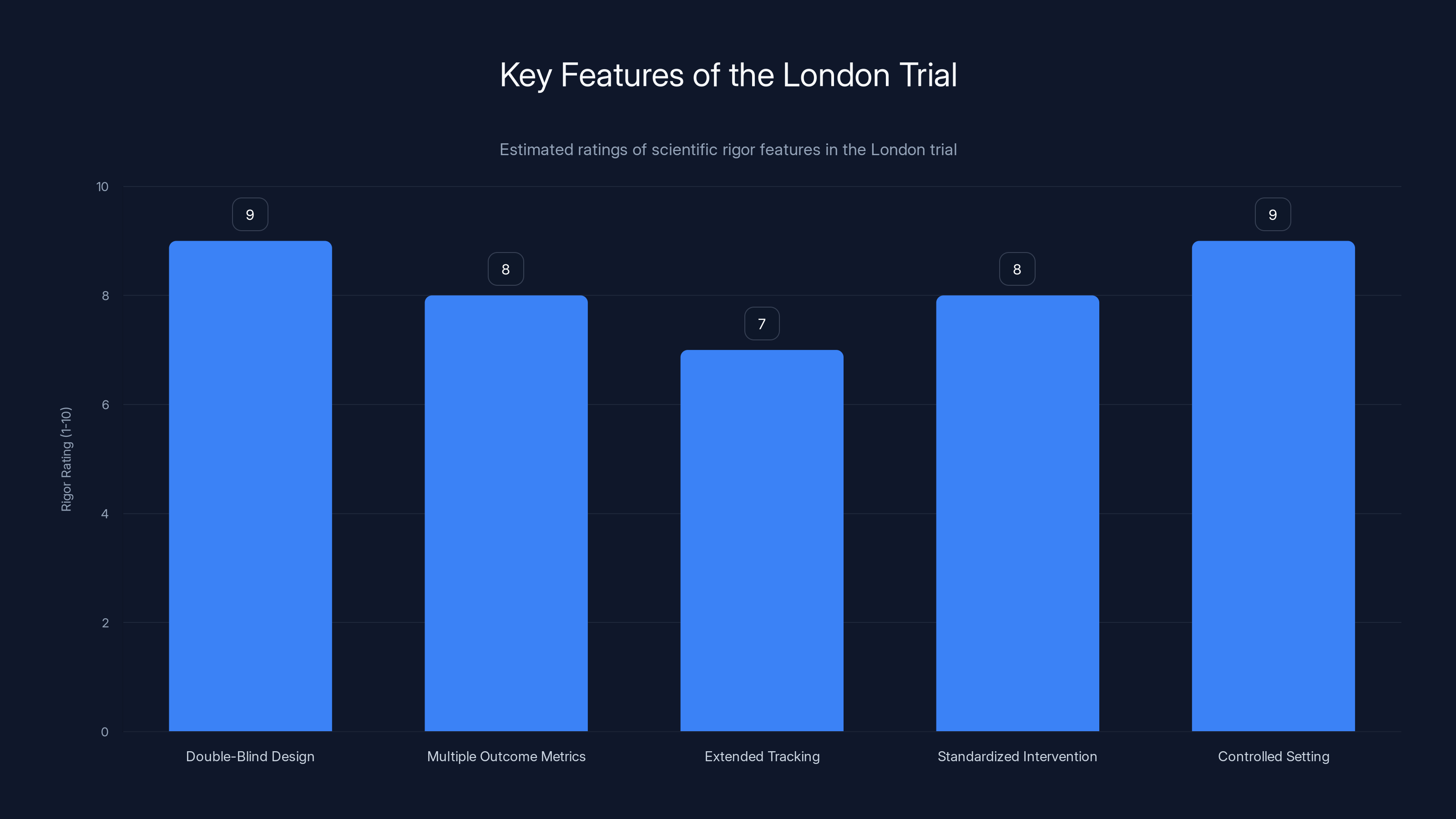
The London trial's scientific rigor is highlighted by its double-blind design and controlled setting, both rated highly for their contribution to reliable results. Estimated data.
How DMT Triggers Neuroplasticity: The Molecular Mechanism
At the molecular level, DMT activates serotonin 2A receptors, but that's only the beginning of a complex cascade. When these receptors fire, they increase glutamate release in the prefrontal cortex. Glutamate is an excitatory neurotransmitter—it makes neurons more likely to fire. This increased neural activity sets off several downstream effects.
First, there's increased expression of growth factors like BDNF, particularly in the hippocampus, a region crucial for memory formation and emotional processing. BDNF is like fertilizer for neurons. It promotes the growth of new neurons in a process called neurogenesis and strengthens connections between existing neurons. Depression is associated with reduced hippocampal volume and reduced BDNF expression—essentially, depression shrinks this region. Psychedelics appear to reverse this.
Second, psychedelics increase something called "thalamocortical filtering." The thalamus acts as a gate, filtering sensory information before it reaches your conscious awareness. Normally, this filtering is quite restrictive—your brain ignores 99% of available sensory information so you can focus. Psychedelics appear to relax this filtering, which explains the sensory intensity and novel perceptual experiences. But they also explain something psychologically important: your brain suddenly processes information in ways it normally doesn't. Habitual thought patterns are disrupted.
Third, there's evidence that psychedelics increase the diversity and independence of neural network activity. Different brain regions that normally communicate in predictable patterns start firing in less synchronized ways. This sounds chaotic, but it's actually therapeutically useful. Depression involves excessive synchronization between the default mode network (associated with self-referential thinking and rumination) and other brain regions. Breaking up this synchronization interrupts depressive thought patterns.
DMT's rapid clearance means these neurochemical effects are compressed into a shorter window, but they're not necessarily weaker. The brain's response seems to involve the same molecular mechanisms as longer-acting psychedelics—BDNF production, enhanced neuroplasticity, increased neural connectivity diversity.
One crucial detail: these neurochemical changes persist long after DMT leaves your bloodstream. This is critical for understanding why a brief drug experience can have lasting effects. The drug triggers a cascade that the brain then maintains. It's like pushing a boulder over a hilltop—the push is brief, but the boulder keeps rolling.
Comparing DMT to Other Psychedelics: Why Speed Matters Clinically
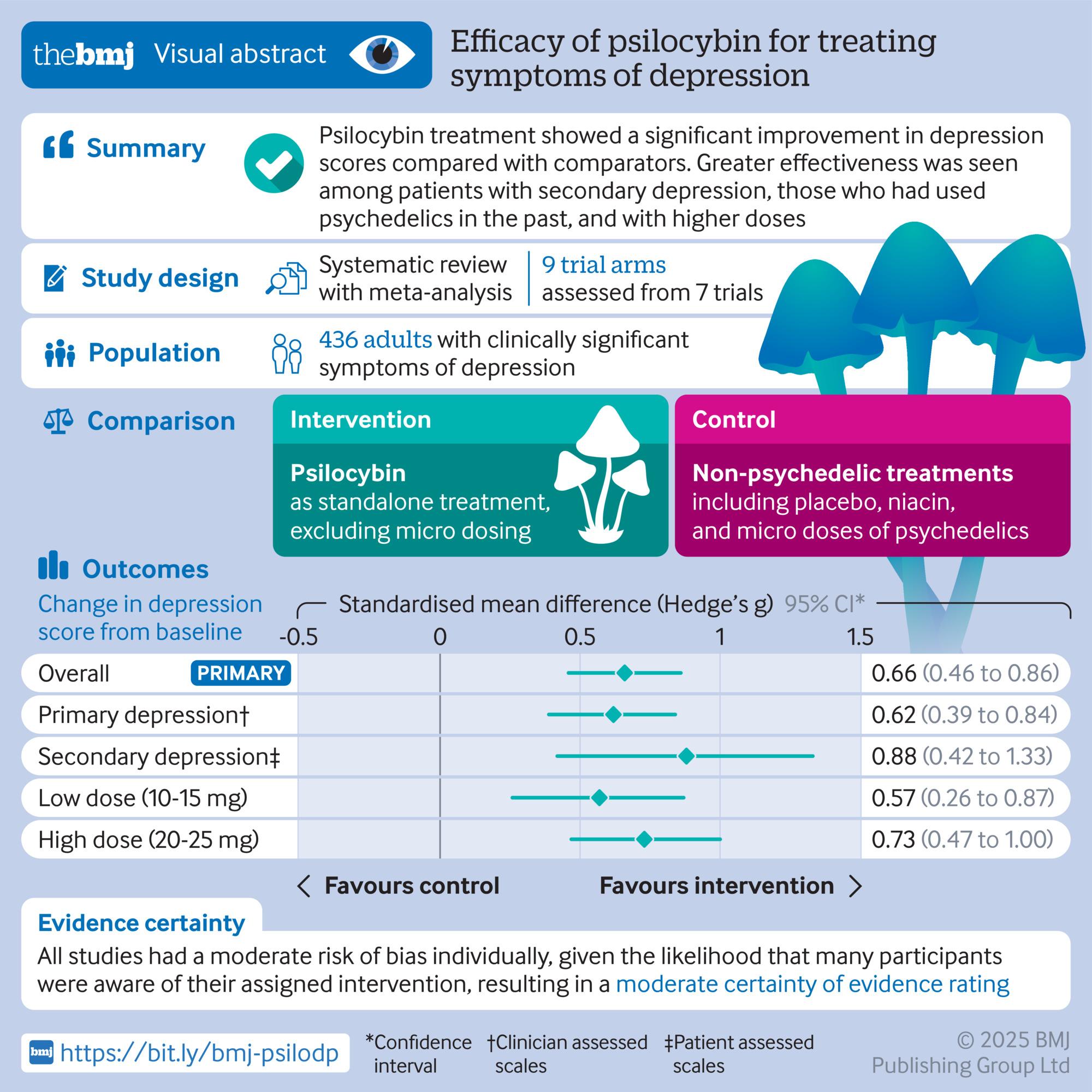
Psilocybin (the active ingredient in magic mushrooms) has received more research attention than DMT, largely because its longer duration—four to six hours—was considered an advantage. A longer experience seemed more likely to produce lasting change. Multiple clinical trials have now shown psilocybin-assisted therapy produces rapid and robust antidepressant effects.
LSD's effects last even longer, typically eight to twelve hours. Both psilocybin and LSD are being pursued by pharmaceutical companies and research institutions as potential depression treatments. Yet both have significant practical limitations. If you're going to give someone LSD as a depression treatment, they need to be monitored and supported for eight to twelve hours. This means dedicated clinical space, trained staff, and a significant time commitment from the patient.
DMT changes this equation entirely. The acute effects last thirty to sixty minutes. Patients are back to baseline consciousness within an hour and a half. From a healthcare logistics perspective, this is transformative. You could potentially offer this treatment in an outpatient clinic. Patients could go home the same day. The resource requirements drop dramatically.
There's an argument that the longer duration of other psychedelics might produce more processing time. More time to have insights, to emotionally work through material, to integrate the experience. But the London trial suggests that the duration of the acute experience doesn't determine the duration of the benefit. Both DMT's brief effects and psilocybin's longer effects produce similar antidepressant outcomes weeks and months later.
This suggests that what matters isn't how long the acute experience lasts but rather the intensity of neuroplasticity it triggers and the psychological processing it catalyzes. DMT seems as good at triggering this as anything else, which is remarkable given its speed of action and clearance.
There's also a practical advantage related to safety monitoring. LSD and psilocybin are usually taken orally, which creates variability in absorption depending on factors like food intake, individual metabolism, and gut health. DMT delivered intravenously produces a more consistent, predictable experience. Medical professionals can titrate the dose and control the timing of onset and offset much more precisely. For clinical purposes, this consistency is valuable.
Safety Profile: What We Know and Don't Know Yet
The London trial found no serious adverse effects following DMT administration. The most common side effects were transient: brief elevations in heart rate and blood pressure, which are common to all psychedelics and usually resolve within minutes. Some participants experienced minor pain at the injection site—a trivial concern.
Psychologically, no one in the trial reported lasting distress or complications from the experience. This is important because psychedelics can theoretically trigger or exacerbate underlying psychiatric conditions in vulnerable individuals. The trial didn't reveal this happening, but it's worth noting that the sample size was small (47 people per group) and participants were screened for certain risk factors like active psychotic symptoms or severe personality disorders.
One concern with any antidepressant is whether it causes dependence. Classic antidepressants like SSRIs can cause physical dependence—abruptly stopping them often produces withdrawal symptoms. Psychedelics appear not to produce dependence in this sense. They don't create withdrawal syndromes. They don't seem to be addictive in the way that alcohol or opioids are, even though their neurochemical effects are powerful.
There's theoretical concern about whether repeated psychedelic experiences could cause long-term brain changes that become problematic. The research so far suggests psychedelics are surprisingly well-tolerated over repeated administrations, but most clinical protocols use single or infrequent doses rather than repeated treatment. The London trial involved two doses: one placebo and one active drug. We don't have extensive data on what happens with monthly or quarterly DMT sessions over years. That's a question future research will need to answer.
Cardiovascular effects deserve specific attention. The brief spikes in heart rate and blood pressure triggered by psychedelics are benign for most people but could theoretically be problematic for someone with uncontrolled hypertension or certain cardiac conditions. This is why screening and medical monitoring matter. The same consideration applies to any powerful psychoactive drug.
Serotonin syndrome—a rare but serious condition that occurs when serotonergic drugs interact—is a theoretical concern, particularly if someone is on an SSRI and receives a psychedelic. However, in the trial, participants weren't on other serotonergic medications at the time of dosing. Clinical protocols would need to carefully manage drug interactions if this treatment enters mainstream use.
The overall safety picture is reassuring, but conclusions must remain tentative. This is a small trial with a short follow-up period. Decades of clinical use might reveal issues that don't appear in a 94-person study. This is why regulatory pathways require larger Phase II and Phase III trials before approving a new psychiatric medication.
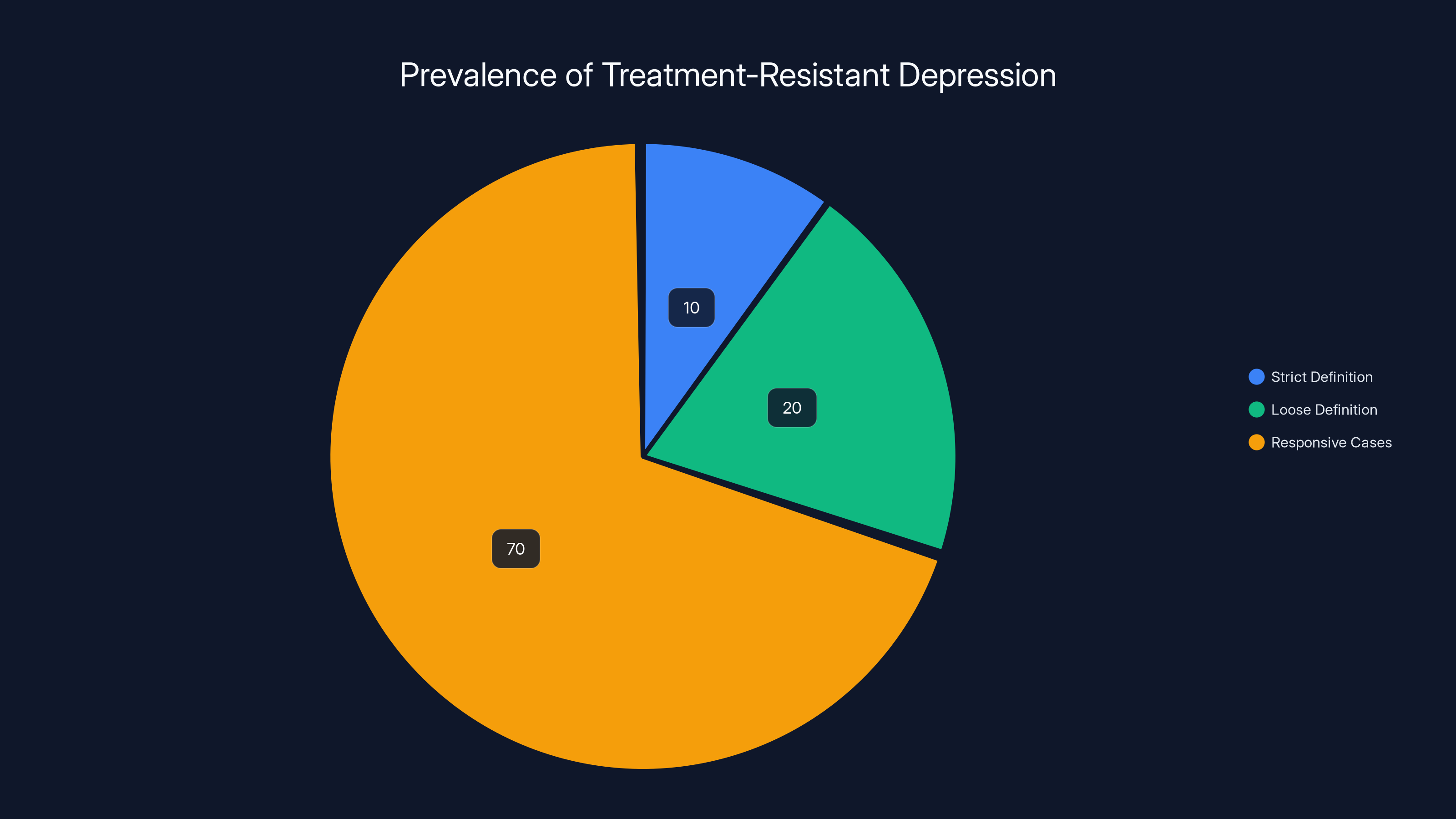
Approximately 10% of depression cases are treatment-resistant under strict definitions, while up to 30% are considered resistant under looser criteria. Estimated data.
The Treatment-Resistant Depression Problem: Why New Options Are Desperately Needed
Treatment-resistant depression affects between 10% and 30% of people with major depressive disorder, depending on how strictly you define "treatment resistance." At the strictest definition—failure to respond to at least two different antidepressants at adequate doses for adequate durations—you're looking at roughly 10% of depressed people. At the looser definition—suboptimal response to available treatments—it's closer to 30%.
This matters because when conventional antidepressants don't work, options become limited and increasingly drastic. You might try combining medications, augmenting with other drugs like antipsychotics, or escalating to interventions like electroconvulsive therapy (ECT). ECT is remarkably effective—it produces rapid antidepressant effects in a high percentage of people—but it requires anesthesia, carries small risks of cognitive effects, and is understandably frightening to patients. Many people would prefer an alternative.
Transcranial magnetic stimulation (TMS) is another option: magnetic coils placed against the scalp stimulate brain tissue. It's noninvasive but requires multiple sessions over weeks, doesn't work for everyone, and the antidepressant effects sometimes fade over time.
Psychotherapy works for some treatment-resistant cases, but when depression is severe and medication-resistant, talking about your feelings while your brain chemistry is fundamentally dysregulated has limited impact. Most people need some biological intervention in addition to or before engaging in meaningful therapy.
This is where psychedelic-assisted therapy becomes relevant. The London trial was recruiting people who had failed conventional treatments. For this population, a single or double dose of DMT that produces meaningful improvement in depression symptoms—without the resource-intensive requirements of eight-hour monitoring—could be genuinely life-changing.
The economic argument is also significant. Depression is expensive. It costs healthcare systems billions in direct treatment costs plus additional billions in lost productivity due to absenteeism and reduced work performance. If a brief psychedelic experience could reduce that burden, the healthcare economics work out favorably even without accounting for the human suffering prevented.
Neuroimaging Evidence: What Brain Scans Reveal About Psychedelic Effects
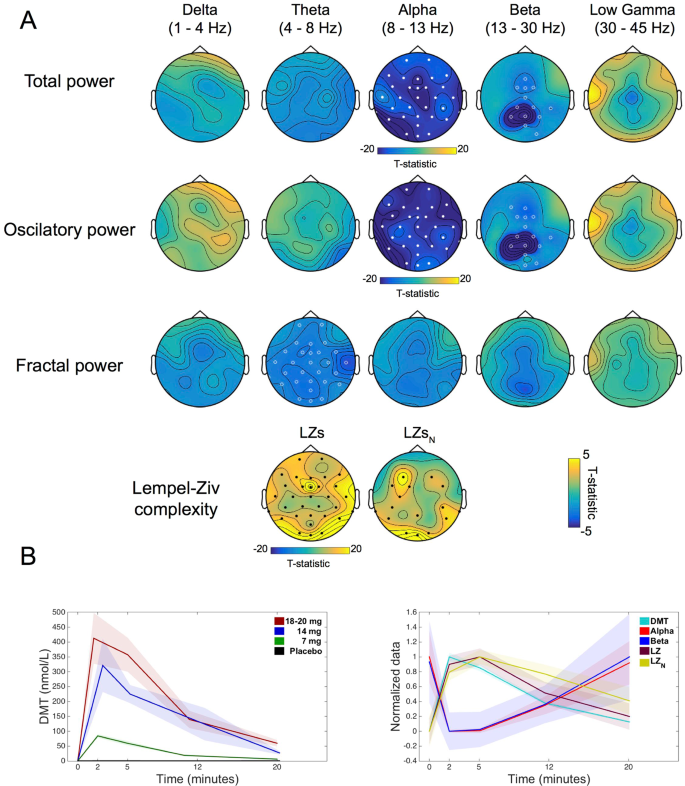
We don't have detailed neuroimaging data specifically from the London DMT trial, but related research using PET and fMRI scans with psilocybin and other psychedelics provides mechanistic insights. These studies show consistent patterns across different psychedelics, suggesting DMT likely works through similar mechanisms.
One striking finding involves the default mode network (DMN), a constellation of brain regions that activate when you're not focused on external tasks—essentially, when you're lost in thought, ruminating, or engaging in self-referential thinking. Depression is characterized by hyperactivity and hypersynchronization within the DMN. Depressed brains are stuck in self-referential loops: thinking about how bad you feel, why you feel bad, what's wrong with you, and how hopeless your future is. This rumination feeds depression.
Psychedelics suppress DMN activity and, crucially, decrease the synchronization between the DMN and other brain networks. The brain stops being locked into this depressive rumination pattern. Simultaneously, connections increase between brain regions that don't normally communicate much—a kind of desegregation of neural networks. This increased diversity and reduced rigidity appears to persist after the acute psychedelic effects wear off.
Another key finding involves something called the salience network, which is responsible for deciding what information deserves your attention. In depression, the salience network becomes dysregulated—depressed people notice threats and negative information preferentially while ignoring positive information. Psychedelics appear to recalibrate this network, at least temporarily. But that temporary recalibration, combined with the increased neural flexibility, seems to produce lasting shifts in how information gets processed.
Functional connectivity studies suggest that psychedelics increase the integration and communication between brain regions that normally operate independently. It's almost as if the usual organizational principle of the brain—where different regions specialize and maintain some functional independence—temporarily breaks down, allowing new patterns of communication to emerge.
When the drug wears off and connectivity patterns normalize, they don't return to exactly their starting configuration. It's like the brain experienced a brief period of chaos that forced a reorganization into a slightly different, more adaptive stable state. Depression represents a particular kind of brain organization—one that maintains depressive thoughts and low motivation. Psychedelics disrupt this organization just long enough for neuroplasticity to install a different configuration.
DMT likely produces similar patterns given its neurochemical mechanism, though we'd need actual neuroimaging studies to confirm this. The fact that behavioral outcomes (antidepressant effects) are comparable between DMT and longer-acting psychedelics suggests the neural changes are likely similar as well.
What Happens After the Acute Experience: Long-Term Brain Changes
The duration of benefit in the London trial is noteworthy. Two weeks after DMT, nearly half the participants reported improvement. Fourteen weeks later, the majority of these improvements persisted. This is particularly striking because DMT's presence in the bloodstream is completely gone within an hour.
How does a brief drug exposure produce benefits that last months? Several mechanisms probably contribute. The first is the neuroplasticity we discussed—the brain's enhanced ability to form new connections. During and shortly after the psychedelic experience, the brain is particularly malleable. If therapy or integration work happens during this window, it gets "written in" with greater neural strength than it would be otherwise.
This is partly why "set and setting" matter so much in psychedelic contexts. Set means your mindset, expectations, and psychological preparation. Setting means the physical and social environment. In the London trial, everyone received counseling. The psychedelic experience didn't occur in isolation but within a therapeutic relationship. This likely matters. The insights or shifts that occur during the psychedelic experience get consolidated through subsequent therapeutic discussion and integration work.
The second mechanism involves what's called the "plasticity window" closing over time. After a psychedelic experience, the brain remains in a heightened plastic state for days or weeks. During this time, new learning and experiences are preferentially integrated into long-term brain organization. Consciously directing attention and activities toward depression-reducing behaviors during this window—maintaining social connections, engaging in activities you value, practicing new thought patterns—gets encoded more durably.
The third involves something more neurochemical. Psychedelics increase BDNF for extended periods. They produce lasting changes in receptor sensitivity. They enhance neuroinflammatory markers that might reduce chronic inflammation associated with depression. These chemical changes don't require the drug to stay in your system. Once triggered, they run their course.
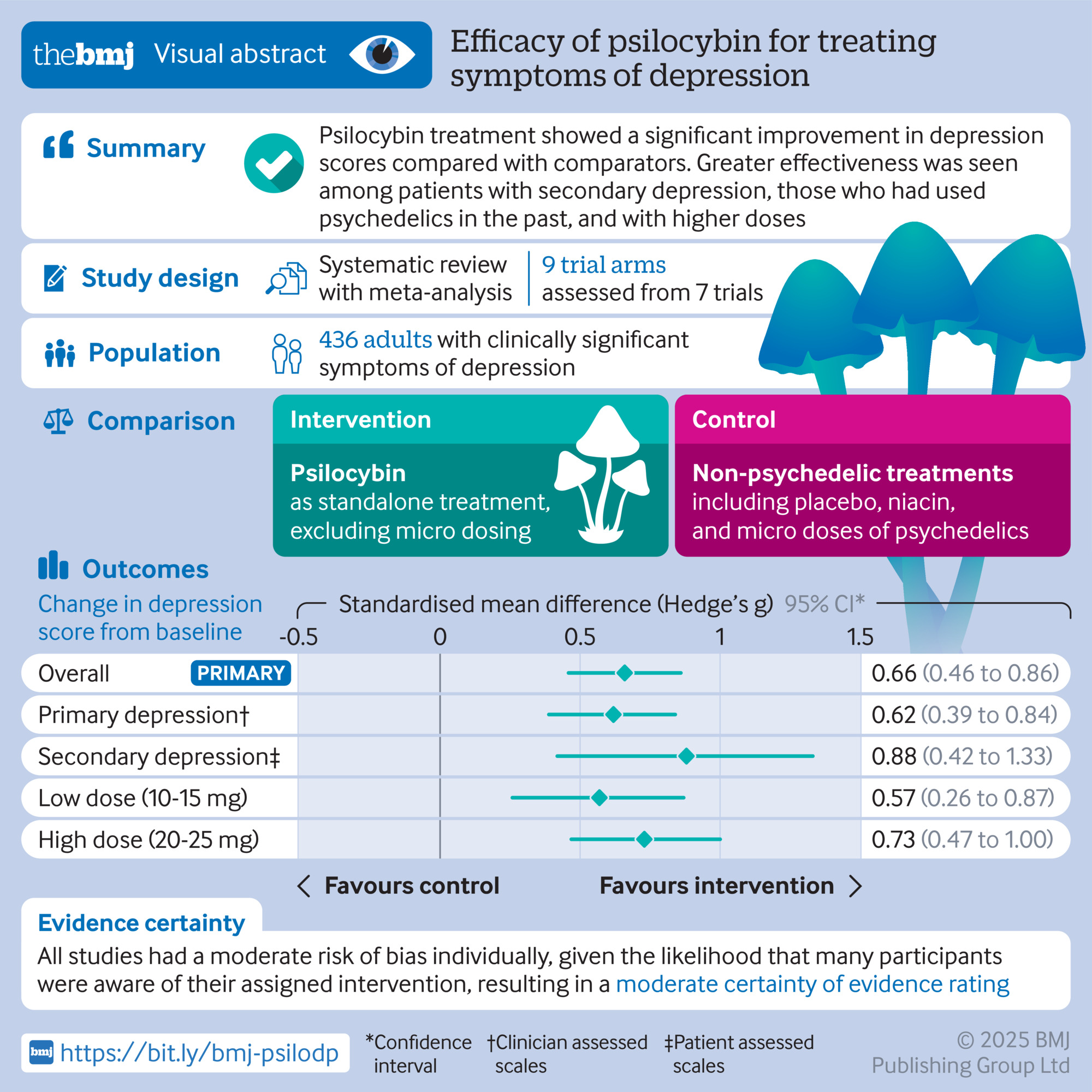
A recent meta-analysis of psychedelic-assisted therapy for depression found that benefits tend to remain stable or even improve slightly over twelve months of follow-up. This isn't what you'd predict if the mechanism was purely acute chemical effect. It suggests that the brain changes triggered by psychedelics and the psychological insights gained during the experience become self-sustaining.

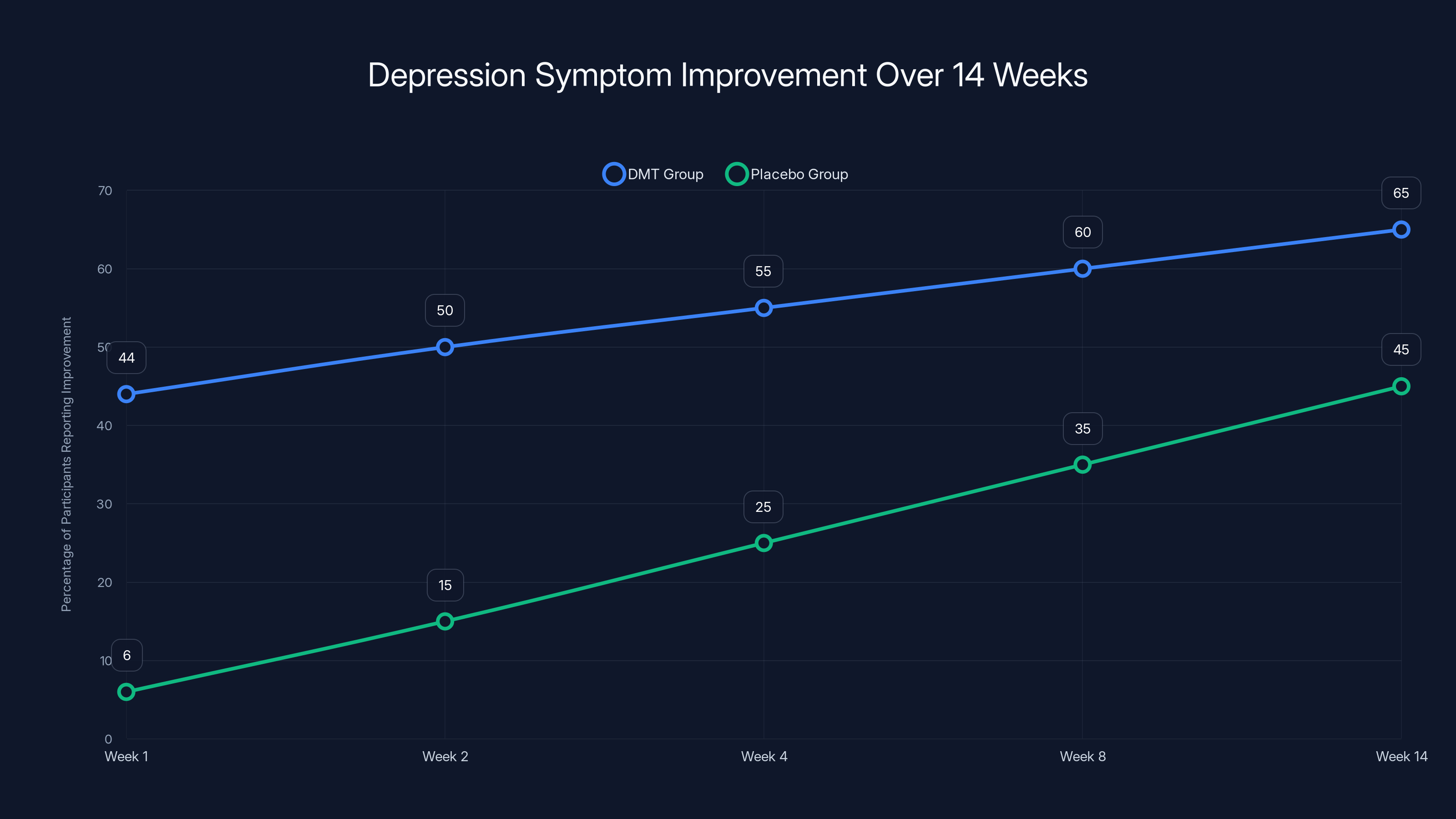
The DMT group showed a significant improvement in depression symptoms, with 44% reporting improvement at week 1, increasing to 65% by week 14. The placebo group improved more gradually, reaching 45% by week 14. Estimated data based on trial description.
Regulatory Pathways: Getting DMT from Research to Clinic
The London trial was a Phase IIb study—early evidence suggesting a treatment works, but not yet definitive proof it's ready for clinical use. The regulatory pathway from here is clear but lengthy. Phase III trials need to be conducted, which typically involve larger sample sizes (hundreds of participants) and longer follow-up periods. These trials need to demonstrate not just that the drug works better than placebo but that it's safe in broader populations.
For psychiatric drugs, the FDA and EMA have specific guidance. You need evidence that benefits persist, that the treatment doesn't produce dependence or abuse potential, that it works in diverse populations, and that rare side effects are identified. This typically takes several years and tens of millions of dollars.
DMT has some regulatory advantages. It's not a novel molecule—it exists naturally in the body, has a long history of use in traditional contexts, and has been studied in research settings for decades. There's no question about whether it's theoretically possible to manufacture safely. There's no question about basic toxicology. The regulatory question is narrower: does it produce clinical benefit for depression specifically, and can this benefit be reliably and safely produced in a controlled clinical setting?
Another regulatory consideration is Schedule status. DMT is currently a Schedule I controlled substance in the United States, meaning it's illegal to manufacture, distribute, or possess without specific government authorization. Psilocybin and LSD have similar status. This creates administrative hurdles for research—you need specific licenses and heavily regulated facilities. However, once a drug shows sufficient clinical benefit through controlled trials, the DEA and FDA can reclassify it or grant special exemptions allowing medical use even if recreational use remains illegal. This has happened with other drugs (cannabis with CBD for specific conditions, for instance).
Several psychedelic therapy companies are actively pursuing regulatory approval for psilocybin-based depression treatments. Some are probably ten years ahead of DMT given their earlier entry into clinical development. But once one psychedelic-based therapy gains approval, the path becomes clearer for others with similar mechanisms.
The timeline is probably five to ten years before DMT-assisted therapy could potentially be available as a medical treatment, assuming Phase III trials are successful. This assumes funding for those trials materializes, which isn't guaranteed. University research typically receives National Institute of Health funding, while private companies fund their own development. Several private companies are focused on psychedelics, so the funding landscape is more favorable than it was five years ago, but still far from guaranteed.

Integration and Therapy: The Psychological Infrastructure That Amplifies Benefits
Neither the London trial nor other psychedelic therapy research shows benefits from the drug alone. Everyone in the therapeutic group received counseling and psychological support. The psychedelic experience is the catalyst, but integration and subsequent therapy appear to be the sustaining structure.
Several models for integration exist. The most common in research settings involves intensive therapeutic support before the psychedelic experience (preparation), professional monitoring during the experience (the actual dosing session), and follow-up therapy sessions afterward to make sense of what occurred and consolidate insights.
What happens during the acute experience itself is fascinating from a psychological perspective. People report their sense of separate self dissolving, ordinary time and space dissolving, and confronting aspects of themselves or existence that feel fundamentally true in a way that contradicts depression's worldview. Depression tells you that suffering is pointless, that nothing meaningful exists, that you're fundamentally broken. These experiences present direct contradiction to those beliefs.
This is where the mystical experience becomes important. People report spiritual insights—feelings of connection to something beyond themselves, of being part of something larger. These experiences are powerful partly because they feel true in the moment in a way that intellectual understanding never could. Someone struggling with depression might intellectually understand that life has meaning, but understanding and deeply feeling are different. The mystical experience seems to involve a shift from intellectual knowing to felt knowing.
Therapists helping people integrate these experiences help them translate the insights into lasting changes. A crucial part is preventing the experience from being isolated or mystified in unhelpful ways. The goal isn't to develop a delusional interpretation of what happened but to extract the genuine psychological insights and consolidate them into how you live.
For example, a person might have an experience of fundamental connection to other humans, experiencing their separateness as an illusion and feeling their interdependence deeply. A good therapist would help translate this into practical behavioral shifts: perhaps initiating reconnection with estranged friends, engaging in more community involvement, or recognizing depression's lie that isolation is necessary. The experience provided the opening; therapy provides the structure for change.
Individual Differences: Who Benefits Most and Why
The London trial showed that roughly 44% of DMT recipients reported meaningful improvement, compared to 6% of placebo recipients. This means most but not all people benefited. Why? Several factors likely matter.
One is baseline psychological openness to the experience. People who approach psychedelics with curiosity and acceptance rather than fear or resistance tend to have more positive experiences and better outcomes. This isn't just about enjoying the experience more—it's about being able to learn from it. Fear and resistance close off psychological processing.
Second is the severity and type of depression. The trial recruited people with treatment-resistant depression specifically. For these individuals, conventional treatments had failed. They may have been more motivated to engage with an unconventional treatment, or they may have had depression with different neurobiological underpinnings that respond better to psychedelic mechanisms than SSRIs.
Third is the mystical experience itself. Remember that antidepressant effects correlated with the intensity of mystical experience as measured by the Mystical Experience Questionnaire. People who had more profound experiences of ego dissolution and spiritual meaning reported better outcomes. This suggests that the depth of the neuroplasticity and psychological shift matters.
Fourth is the quality of therapeutic support. While the trial provided counseling to everyone, the quality and depth of that support probably varied. People with better therapeutic relationships likely benefited more from the combination of psychedelic and therapy.
Fifth involves what might be called "psychological readiness." Depression is stable partly because it's self-reinforcing—depressed thoughts and low motivation make it hard to engage in activities that would improve mood. Some people are more ready to break this cycle than others. The psychedelic experience provides a window, but people still need to walk through it. Those who actively work during the integration period likely do better.
This points to an important distinction. Psychedelic therapy isn't simply about taking a drug and getting better. It's an intervention that requires psychological engagement. People who are passive or who use it as a substitute for engaging with their own psychology might get less benefit. The most successful outcomes probably involve people who see the psychedelic as a tool that opens possibility, then actively work to build on that opening.
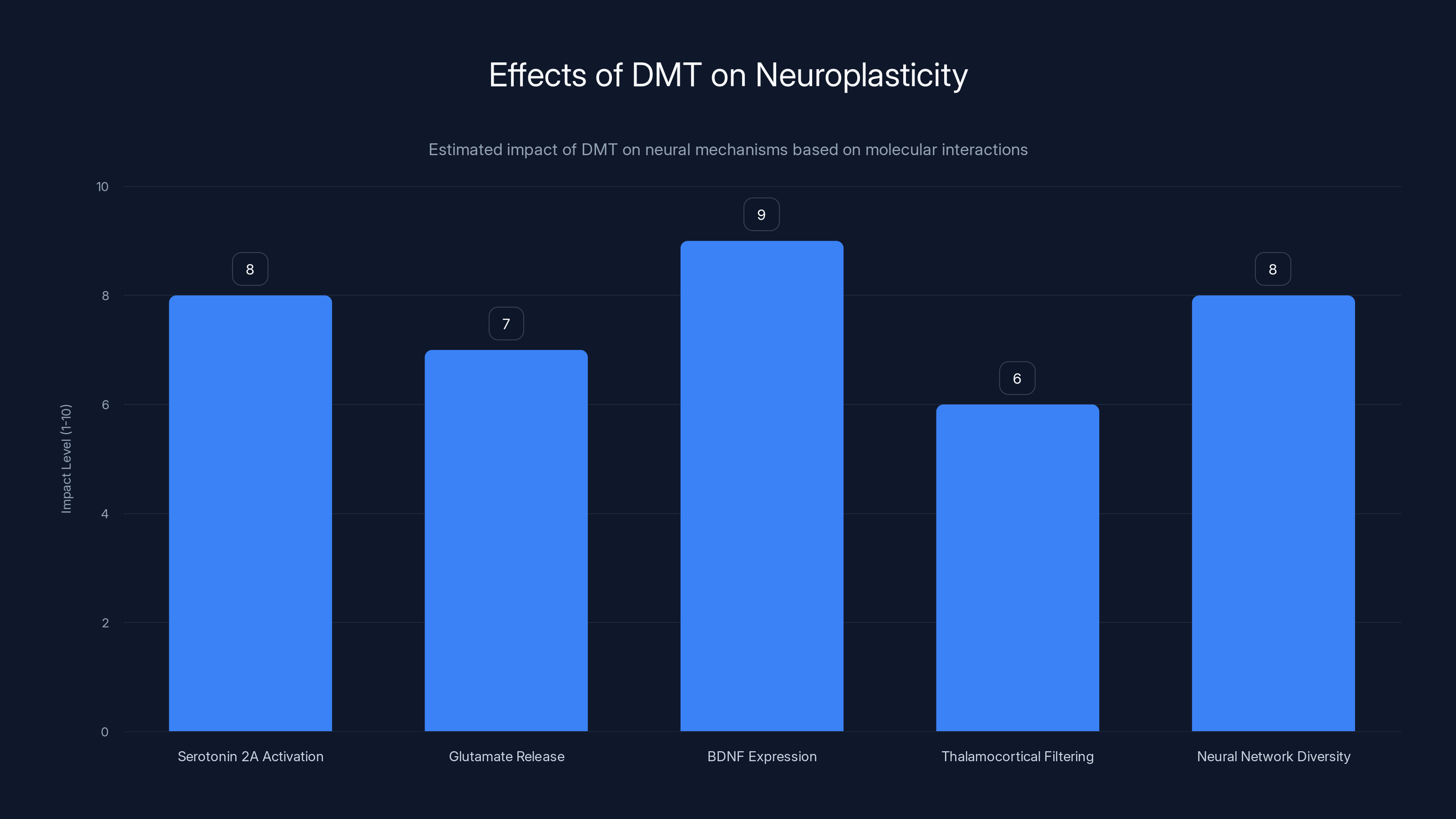
DMT significantly influences neuroplasticity by activating serotonin receptors, increasing glutamate and BDNF, altering sensory filtering, and enhancing neural network diversity. Estimated data.
Comparing to Traditional Antidepressants: When and Why You'd Choose Each
SSRIs, SNRIs, and other conventional antidepressants remain the first-line treatment for depression. They have the advantages of being well-studied over decades, widely available, relatively inexpensive, and effective for many people. They're taken daily, which provides continuous neurochemical support. For people who respond, they work well.
Psychedelic-assisted therapy targets the subset of people who don't respond adequately to conventional treatments. They're not meant to replace SSRIs but to provide an option when SSRIs fail. This is a crucial distinction. No one is suggesting depressed people start with psychedelics. The regulatory development is targeting treatment-resistant populations specifically.
The mechanisms are also quite different. SSRIs work primarily by increasing available serotonin through blocking reuptake—essentially, making what serotonin your brain produces last longer. Psychedelics work by activating specific receptors that trigger neuroplasticity and force psychological processing. These aren't competing mechanisms—they address depression through different pathways.
There's an interesting possibility for future combinations. What if someone was partially responsive to an SSRI—not depressed, but not fully recovered—and received a single dose of DMT while continuing their SSRI? The SSRI would provide ongoing neurochemical support, while the psychedelic would trigger the plasticity and integration process. Some researchers are exploring this possibility, though no robust data exists yet.
Another consideration is the side effect profile. SSRIs often take weeks to work and frequently cause side effects—sexual dysfunction is common, weight gain or loss, emotional blunting (feeling less), or activation effects (anxiety, insomnia). Psychedelics produce acute perceptual and psychological effects that are transient and, in most cases, not experienced as negative. The tradeoff is that SSRIs work every day while psychedelics work once or twice.
Cost is another factor. A month of SSRI medication might cost fifty to two hundred dollars depending on the drug and insurance. A psychedelic therapy session including the drug, clinical monitoring, and therapeutic support might cost several thousand dollars. This is more expensive per occurrence, but if it produces lasting benefits from just one or two doses, the per-unit cost over time might be competitive.
Future Research: What Questions Remain Unanswered
While the London trial is encouraging, it represents just one step in the research process. Several critical questions remain. Does DMT work for depression in people who haven't failed conventional treatment? Would it work better for certain subtypes of depression? How many doses are optimal—is one dose enough, or do people benefit from multiple doses spaced over months?
Do different preparation and integration protocols produce different outcomes? The trial used a relatively standardized counseling approach, but psychedelic therapists have developed more intensive and elaborate integration protocols. Would these produce better or longer-lasting benefits?
How durable are the benefits over years? The trial followed people for 14 weeks. What happens at six months, one year, five years? Do people maintain benefit, or does depression gradually return? If it returns, can it be treated again with repeat doses?
How does DMT compare directly to psilocybin or other psychedelics in head-to-head trials? The assumption is that all psychedelics work through similar mechanisms and produce similar benefits, but this hasn't been definitively tested. Maybe DMT's rapid action produces qualitatively different or superior outcomes compared to longer-acting psychedelics.
What is the mechanism of the mystical experience itself, and can it be enhanced or predicted? If antidepressant effects depend on the intensity of mystical experience, understanding what determines that intensity could improve treatment outcomes.
Can psychedelic therapy be improved through combining it with other interventions? For example, what if someone received DMT followed by a week of intensive daily therapy, or DMT combined with light therapy, or DMT with specific cognitive-behavioral exercises?
What's the optimal therapeutic approach for people who don't have a mystical experience? Some portion of people receiving psychedelics don't report profound spiritual experiences. Do they benefit less, and if so, what else could help them?
The Bigger Picture: Why This Matters for How We Understand Mental Illness
The DMT trial and related research fundamentally challenge how we understand depression. The conventional model treats depression as a chemical imbalance, primarily a serotonin or norepinephrine problem that needs correction with daily medication. This model has merit—SSRIs do work for many people—but it's incomplete.
The psychedelic data suggests that depression involves neurological rigidity and maladaptive neural organization that can be reset through a brief but intense neuroplasticity event. Rather than seeing depression as a purely chemical problem requiring chemical correction, we might see it as a problem of stuck brain organization that can be unstuck under the right conditions.
This shifts the therapeutic focus. Instead of just correcting neurochemistry, we're restoring the brain's ability to change. Instead of sustaining a particular chemical state indefinitely, we're triggering transformation. Instead of suppressing symptoms, we're addressing the underlying neurobiological substrate of depressive patterns.
This also changes our understanding of the mind-brain relationship. Depression isn't just brain chemistry affecting mind. Depression is a psychosomatic phenomenon where thought patterns, meaning systems, and neurobiological organization reinforce each other. Breaking into one level of this system can trigger changes at other levels. A mystical experience—which is fundamentally a mental phenomenon—can trigger lasting neurobiological changes. This is exactly what we'd expect if mind and brain are aspects of one system rather than separate entities that interact only superficially.
For patients, this shift in understanding can be liberating. Depression often involves a sense of hopelessness and permanence—feeling broken in a way that can't be fixed. Evidence that a brief intervention can produce lasting improvement suggests that this permanence isn't inherent to depression. Change is possible. The brain is capable of reorganization. This possibility itself becomes therapeutic.

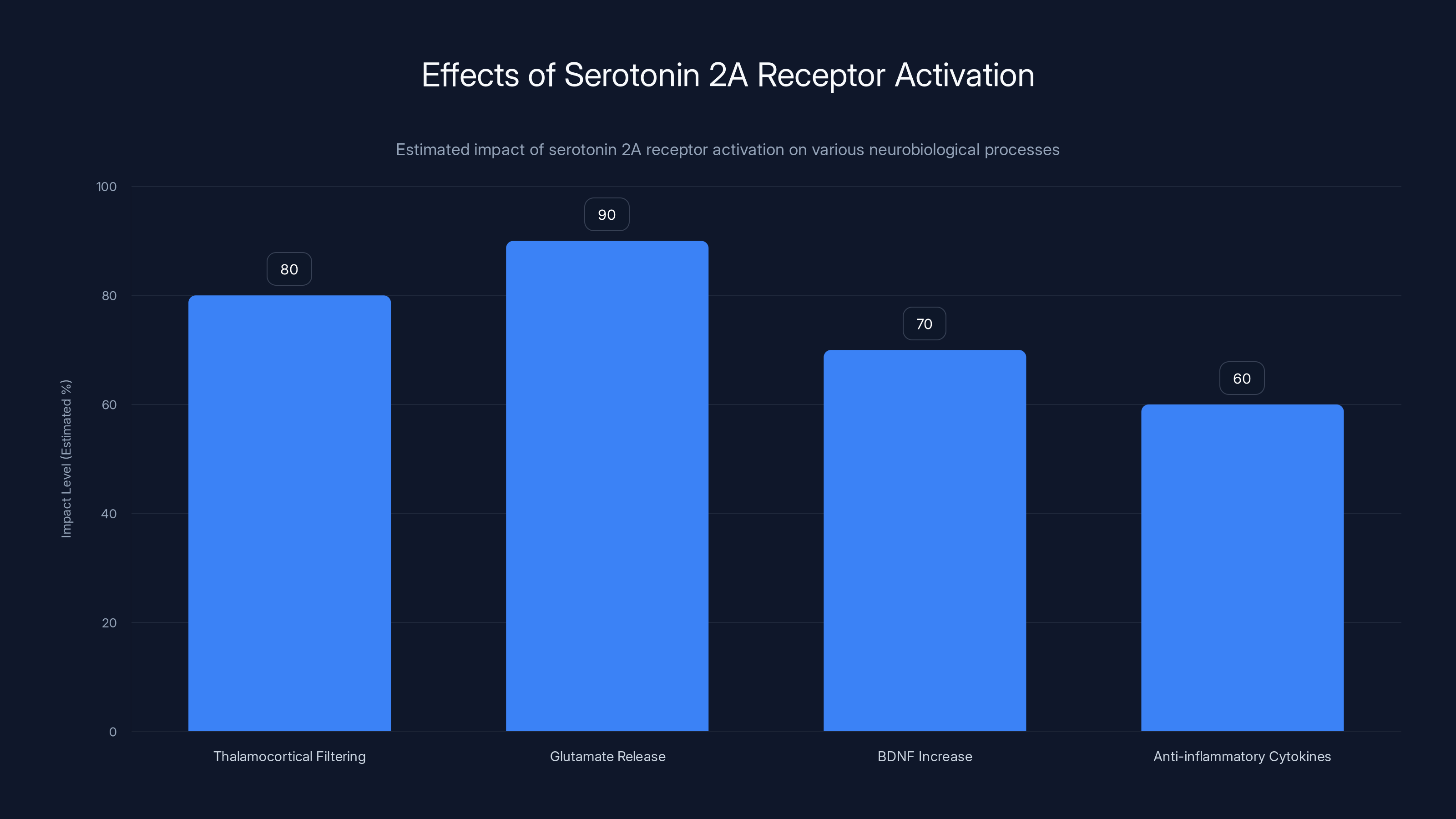
Activation of serotonin 2A receptors significantly impacts glutamate release and thalamocortical filtering, contributing to neuroplasticity and potential antidepressant effects. Estimated data.
Practical Considerations: If This Becomes Available, What Would It Look Like?
Assuming DMT-assisted therapy eventually gains regulatory approval, what would actually using it look like for a patient? The most likely model, based on existing psychedelic therapy research and practice, would involve several phases.
First, screening and preparation. You'd meet with a psychiatrist to confirm treatment-resistant depression and rule out contraindications (severe cardiovascular disease, certain psychiatric conditions like active psychosis, etc.). You'd meet with a psychedelic therapist to discuss what to expect, address fears, explore your intentions and what you hope to gain. You'd likely do preparation work, possibly including meditation or other practices to develop psychological stability.
Second, the actual dosing session. You'd arrive at a clinical setting, likely with a trusted support person or therapist present. You'd receive DMT intravenously over a couple of minutes, then experience thirty to sixty minutes of intense altered consciousness. Professional staff would monitor vital signs and provide reassurance. The therapist would likely be physically present but mostly silent, intervening only if needed for safety.
Third, immediate post-acute phase. After the acute effects wear off, you'd likely rest and be monitored for another hour or so. You might debrief with your therapist, though often the processing begins rather than concludes in this immediate period.
Fourth, integration work. Over the following weeks, you'd meet regularly with your therapist to process the experience, extract meaning, and translate insights into actual behavioral and cognitive change. This is where the real work happens—moving from the powerful memory of the experience to durable changes in how you live.
Fifth, follow-up dosing. Some protocols involve a second dose after a month or longer. This might amplify benefits or address aspects that the first dose didn't fully address.
The entire process from initial consultation to completing integration might take three to six months. The costs would likely be in the thousands—probably somewhere between three thousand and ten thousand dollars depending on the location, provider, and intensity of therapeutic support. Many insurance companies don't currently cover psychedelic therapy since it's not yet FDA-approved, though this could change once regulatory approval occurs.

Real Talk: Hype vs. Reality
It's important to be realistic about what this research shows. A single 94-person trial, while well-designed, isn't definitive proof that DMT is a game-changer for depression. Larger trials are needed. Longer follow-up is needed. Replication in different settings and with different populations is needed.
It's also important to acknowledge that psychedelic therapy isn't universally effective. Not everyone benefits. Some people have difficult experiences that don't obviously translate into psychological benefit. Some people respond initially but don't maintain benefits over time. There's no treatment that works for everyone.
There's also a tendency in both positive and negative directions to oversell psychedelic research. Enthusiasts present it as a magic solution, while skeptics dismiss it entirely. The truth is more nuanced. For some people with treatment-resistant depression, available evidence suggests a psychedelic experience coupled with therapy can produce meaningful and lasting improvement. This is genuinely significant. But it's not a cure-all, and it shouldn't be assumed to work for every depressed person or every subtype of depression.
There are also legitimate concerns about uncontrolled psychedelic use or therapy conducted by untrained practitioners. Psychedelics are powerful and can be psychologically destabilizing if misused or used without proper support. The responsible pathway involves rigorous clinical research, regulatory oversight, and professional training of practitioners. The exciting research results shouldn't be used to justify recreational use or poorly supervised "therapy."
But within those caveats, the evidence is genuinely encouraging. For the subset of people with treatment-resistant depression, it offers hope in a way that existing treatments haven't provided. That's significant.

What Makes the London Trial Scientifically Rigorous
The London trial incorporated several design features that strengthen confidence in the results. It used a double-blind comparison group, acknowledging while not pretending the placebo was perfect. It measured multiple outcome metrics rather than relying on single-symptom assessment. It tracked outcomes over an extended period (14 weeks), not just immediately after dosing. It measured not just symptom reduction but also specific psychological factors (mystical experience) that predicted outcomes.
The sample, while small, was carefully selected. Participants had documented treatment-resistant depression, had failed conventional treatments, and met specific inclusion criteria. The intervention was standardized—everyone received the same dose, delivery method, and monitoring protocol. The clinical setting was controlled, with professional staff providing consistent care.
One limitation is the relatively short follow-up period. Fourteen weeks is barely three months. For a drug treatment, this is actually reasonable, but longer follow-up would be more convincing. Another limitation is the sample size. Ninety-four participants total is sufficient for an early efficacy trial but small for definitive proof. A Phase III trial would likely involve several hundred participants.
The study also measured adverse effects actively rather than just asking if anyone had problems. This is important because mild or transient side effects might be overlooked in less careful assessment.
What's absent from the published trial data is information about what specifically happened in the counseling sessions, how intensively participants engaged in integration work, whether outcomes correlated with the quality of therapeutic relationship, and detailed analysis of what participants with better outcomes did differently. These details would help understand the mechanism and identify ways to improve outcomes.
Neurobiological Mechanisms: The Serotonin 2A Receptor and Beyond
Most classical psychedelics, including DMT, work primarily through serotonin 2A receptors. These receptors are abundant in the cortex, and their activation seems to be the common pathway through which psychedelics produce their characteristic effects. But knowing the receptor doesn't explain the antidepressant effect.
After serotonin 2A activation, several downstream effects cascade. There's increased thalamocortical filtering disruption—essentially, the brain's normal gatekeeping function loosens, allowing more information to reach consciousness. There's also increased glutamate release in key brain regions, which activates neurons and sets off neuroplasticity cascades.
The increased glutamate activity triggers several important signals. It increases BDNF, as mentioned. It also activates specific transcription factors that alter gene expression in neurons, changing what proteins they produce. Some of these proteins are structural—they form the physical basis of neural connections. Others are signaling molecules that facilitate new connection formation.
Additionally, psychedelics seem to increase anti-inflammatory cytokines and decrease pro-inflammatory ones. Chronic inflammation is increasingly recognized as involved in depression. Some antidepressant drugs work at least partly through anti-inflammatory mechanisms. Psychedelics might be adding an anti-inflammatory effect to their direct neuroplasticity effects.
Interestingly, the hallucinogenic and antidepressant effects don't require the same mechanism. You could theoretically block the hallucinogenic effects while preserving the antidepressant ones if you could target specific receptor subtypes. Some researchers are exploring this, though it hasn't proven successful yet. The evidence from the London trial suggests that the hallucinogenic and therapeutic effects are linked—people with stronger hallucinogenic experiences had better outcomes. This suggests they share enough mechanistic overlap that separating them might be difficult.

Conclusion: A New Option for an Old Problem
The London DMT trial adds meaningful evidence to a growing body of research suggesting that psychedelics can produce rapid and lasting antidepressant effects. DMT's particular advantage—its brief duration of acute effects—makes it potentially more practical for clinical implementation than longer-acting psychedelics.
For people with treatment-resistant depression, people for whom conventional antidepressants have failed or produced unacceptable side effects, this research offers hope. Not guaranteed success, but a genuine possibility of significant improvement from a single or double dose of medication combined with professional therapeutic support.
The mechanism is fascinating precisely because it suggests that depression isn't simply a chemical imbalance requiring permanent chemical correction. Instead, it represents a neurobiological state of rigidity that can be disrupted and reset. A brief but intense experience of altered consciousness, processed through psychotherapy, can trigger lasting changes in brain organization and subjective experience.
This reframes what psychological treatment can do. Rather than suppressing symptoms indefinitely, we can catalyze transformation. Rather than seeing depression as a permanent condition to be managed, we can address the neurobiological basis of depressive patterns.
Large Phase III trials are now underway for various psychedelic treatments. Regulatory pathways are becoming clearer. The question isn't whether psychedelics show promise—the research increasingly confirms they do. The question now is how to safely and effectively bring these treatments to patients who need them while maintaining appropriate scientific rigor and oversight.
The journey from research finding to clinical reality typically takes years. But for people suffering with depression that doesn't respond to current treatments, the promise of meaningful help emerging from this research area is genuinely welcome.
FAQ
What is DMT and how is it different from other psychedelics?
DMT (dimethyltryptamine) is a naturally occurring compound found in small amounts in the human brain and certain plants. Unlike psilocybin (lasting four to six hours) or LSD (lasting eight to twelve hours), DMT's acute effects last only 30 to 60 minutes, making it much briefer acting. Despite its short duration, clinical trials suggest it produces comparable antidepressant effects to longer-acting psychedelics, likely because the lasting therapeutic benefit comes from triggered neuroplasticity rather than the duration of acute consciousness alteration.
How does DMT help with depression?
DMT appears to work by activating serotonin 2A receptors, which triggers a cascade of neurobiological changes including increased production of brain-derived neurotrophic factor (BDNF), enhanced neural plasticity, and disruption of the rigid thought patterns characteristic of depression. The psychedelic experience itself—particularly the sense of mystical experience and ego dissolution—seems integral to the therapeutic effect. The brain's heightened malleability during and after the experience allows psychological insights from therapy to take deeper root, producing lasting changes in mood and thought patterns.
What did the London clinical trial actually show?
The study involved 94 people with treatment-resistant depression randomly assigned to receive either DMT or placebo, combined with counseling. One week after dosing, 44% of those receiving DMT reported meaningful improvement in depression symptoms compared to only 6% in the placebo group. At 14 weeks post-dosing, the improvements in the DMT group remained substantially maintained. Importantly, antidepressant benefits correlated with the intensity of the mystical experience participants reported, suggesting the psychological depth of the experience matters for outcomes.
Is DMT-assisted therapy safe?
In the London trial, no serious adverse effects occurred following DMT administration. The most common temporary effects were brief elevations in heart rate and blood pressure, minor injection site pain, and no lasting psychological complications. However, this was a small trial with short follow-up. People with certain cardiac conditions or active psychotic symptoms would be excluded from treatment. Safety monitoring during administration is essential, and the treatment should only be pursued under medical supervision with proper screening.
How long do the antidepressant effects last after a single dose?
In the London trial, benefits observed one week after dosing persisted through 14 weeks of follow-up, though some effect size reduction occurred over that period. Research on longer-acting psychedelics suggests benefits can last six months or longer in many cases. However, long-term follow-up studies extending beyond one year are still limited. Most evidence suggests that integration work and continued psychological engagement during the weeks following treatment helps sustain benefits.
When might DMT therapy become available as a treatment?
DMT is currently in Phase II clinical trials, meaning early efficacy has been demonstrated but larger Phase III trials are needed before regulatory approval. Assuming funding materializes and Phase III trials are successful, the timeline for FDA approval is likely five to ten years. Several psychedelic therapy companies are pursuing regulatory approval for related treatments, which may accelerate the pathway. Once one psychedelic-based therapy gains approval, approval for similar therapies becomes more feasible.
How does DMT therapy compare to traditional antidepressants like SSRIs?
Traditional antidepressants like SSRIs work by maintaining consistent neurochemical changes and are taken daily indefinitely. DMT-assisted therapy involves one or two doses that trigger neuroplasticity and psychological transformation. SSRIs are well-established first-line treatments for depression. DMT therapy appears most promising for people who don't adequately respond to conventional antidepressants. The mechanisms differ significantly—SSRIs provide ongoing chemical support while psychedelics trigger temporary but intense neural reorganization with lasting effects.
Is the mystical experience necessary for antidepressant benefits?
The London trial found that antidepressant effects correlated strongly with the intensity of reported mystical experience and ego dissolution. This suggests the psychological depth of the experience contributes meaningfully to outcomes. However, this doesn't necessarily mean that people without mystical experiences benefit less—they might simply report their beneficial changes differently. More research specifically examining this question would be valuable.
Could someone take DMT therapy while on other antidepressants?
This is an important question still being researched. Combining DMT with SSRIs or other serotonergic drugs theoretically carries risks, though serotonin syndrome appears rare with psychedelics. Most clinical protocols have participants discontinue certain medications before psychedelic treatment. The optimal approach likely varies depending on the specific medications and individual circumstances. Any consideration of combining treatments should only occur under medical supervision.
What percentage of people with treatment-resistant depression benefit from psychedelic therapy?
In the London trial, 44% of DMT recipients reported meaningful improvement, significantly more than the 6% placebo rate. However, this means some people don't achieve meaningful benefit. Outcomes likely vary based on individual factors including psychological openness, severity of depression, therapeutic relationship quality, and post-treatment engagement with integration work. Larger trials with diverse populations will better clarify benefit rates and identify which patients are most likely to respond.
Could psychedelics work for mild depression or as a preventive treatment?
Current research targets treatment-resistant cases where conventional treatments have failed. Whether psychedelics would benefit people with mild depression or serve as preventive treatment hasn't been studied. It seems unlikely they'd be used as first-line treatment given the logistical requirements and potential risks, plus the effectiveness of existing treatments for milder cases. Future research might explore these applications, but currently the clinical justification is strongest for treatment-resistant populations.

Key Takeaways
- DMT produces antidepressant effects comparable to longer-acting psychedelics despite its 30-60 minute acute duration, suggesting lasting neurobiological change rather than temporary symptom suppression
- In the London clinical trial, 44% of treatment-resistant depression patients receiving DMT reported meaningful improvement one week after dosing, with benefits persisting through 14-week follow-up versus 6% in placebo group
- Antidepressant benefits correlated strongly with intensity of mystical experience and ego dissolution, suggesting the psychological depth of the psychedelic experience contributes essentially to therapeutic outcomes
- DMT works by activating serotonin 2A receptors, triggering production of brain-derived neurotrophic factor (BDNF) and enhanced neuroplasticity that persists long after the drug clears the bloodstream in minutes
- Regulatory approval timeline for DMT-assisted therapy is likely 5-10 years away pending larger Phase III trials, but psychedelic therapy represents a genuinely promising option for the estimated 10-30% of depressed people who don't respond to conventional antidepressants

