![Why 99% of Adults Over 40 Have Shoulder 'Abnormalities' on MRI [2025]](https://tryrunable.com/blog/why-99-of-adults-over-40-have-shoulder-abnormalities-on-mri-/image-1-1771339008096.jpg)
The MRI Paradox That's Redefining Shoulder Pain Diagnosis
Imagine getting an MRI for shoulder pain and discovering something "abnormal." Your doctor uses the word "tear." You hear "damage." You think "surgery." But here's the thing: you might be perfectly fine.
That's not pessimism. That's what the research actually shows.
In early 2025, a landmark study published in JAMA Internal Medicine found something that's forcing doctors to rethink how they diagnose shoulder problems. Researchers scanned 602 adults aged 41 to 76 with MRI machines and discovered that 99% of them had at least one rotator cuff abnormality. Tears, tendon thickening, fraying—you name it, they had it.
But here's the kicker: 82% of these people had absolutely no shoulder symptoms. No pain. No weakness. No problems at all.
This finding upends everything we thought we knew about shoulder imaging. It reveals a massive gap between what an MRI shows and what actually matters clinically. And it's happening in clinics worldwide, leading to unnecessary treatments, escalating healthcare costs, and patient anxiety that could have been prevented.
The problem isn't the imaging technology itself. The problem is how we interpret it, what we tell patients, and the cascade of decisions that follow from words like "tear" and "abnormality."
Let's break down what the science actually reveals, why this matters so much, and what you should know if you're facing shoulder pain or considering getting an MRI.
TL; DR
- Nearly all adults over 40 have rotator cuff abnormalities on MRI, yet most are completely asymptomatic.
- The study found no meaningful difference in abnormality rates between symptomatic and asymptomatic shoulders when researchers adjusted for other factors.
- Language matters: Calling normal age-related changes "tears" creates unnecessary anxiety and drives overtreatment.
- Clinical exam and function matter more than imaging findings when deciding on treatment.
- Watchful waiting and physical therapy should be first-line approaches for non-injury-related shoulder pain, not immediate imaging.
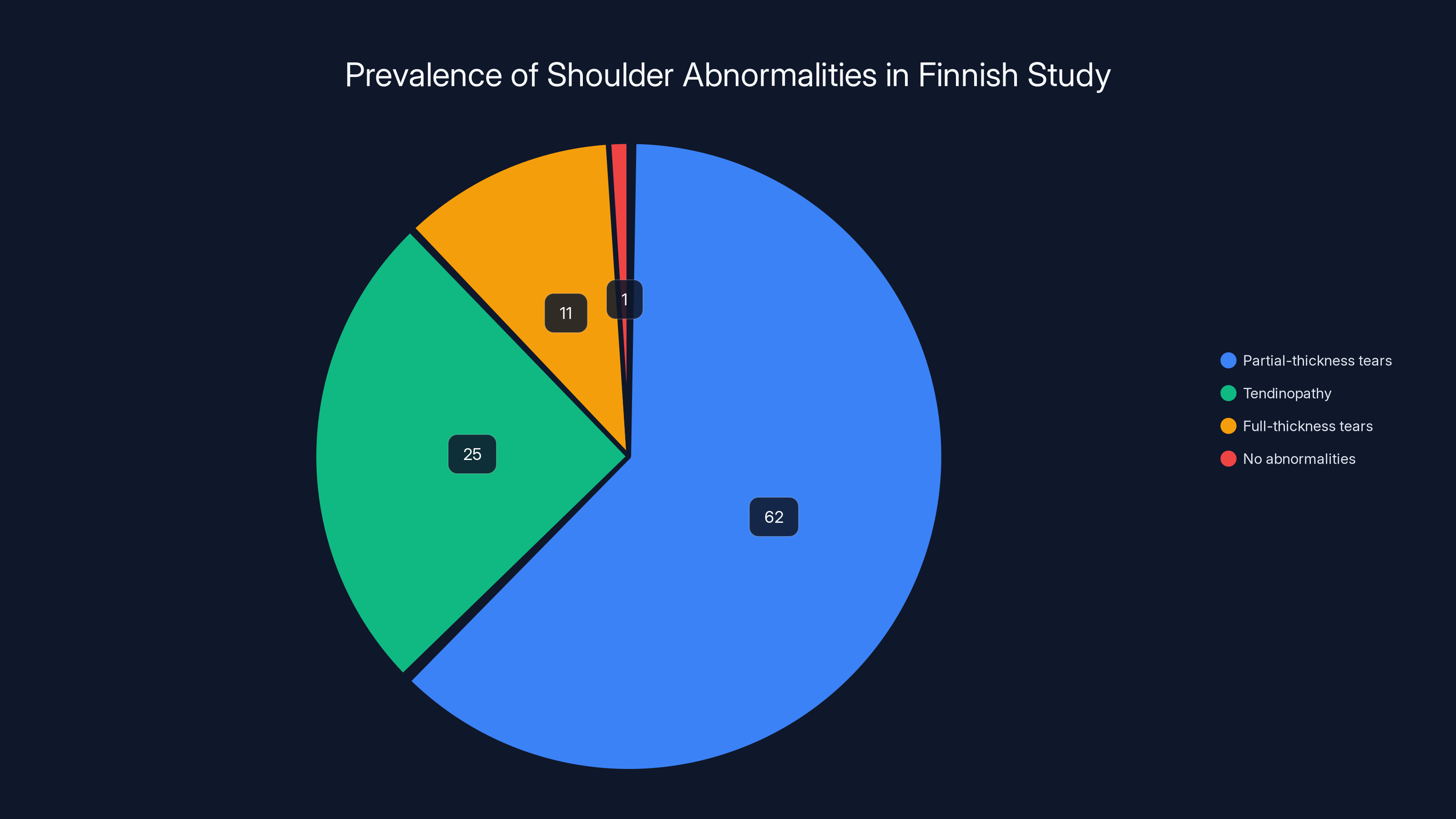
Partial-thickness tears were the most common abnormality, affecting 62% of participants, while 99% had some form of rotator cuff abnormality.
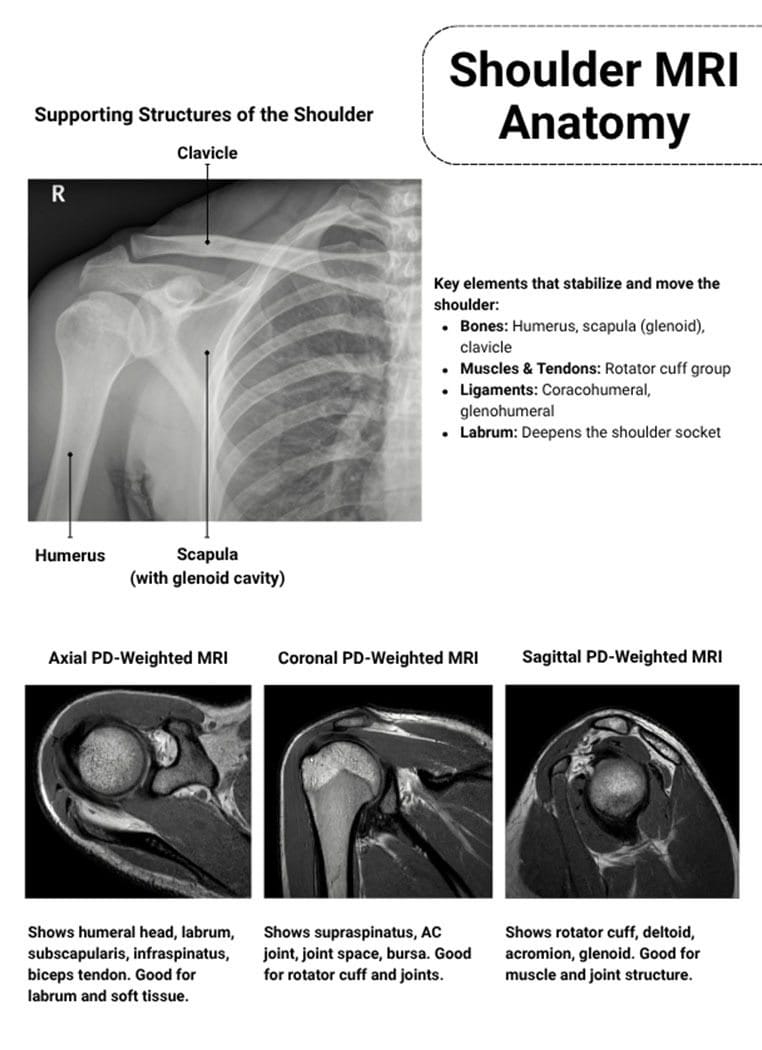
Understanding the Rotator Cuff: What It Actually Does
Before we talk about abnormalities, let's understand what we're actually looking at.
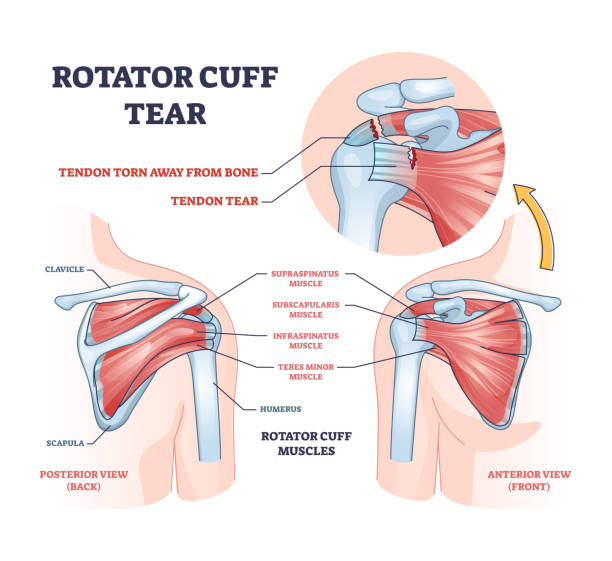
Your rotator cuff isn't one thing. It's a group of four muscles and their tendons that work together to stabilize your shoulder joint. Think of it like a muscular cuff surrounding the ball-and-socket joint of your shoulder, keeping the upper arm bone (humerus) centered in the socket (glenoid).
The four muscles are the supraspinatus, infraspinatus, teres minor, and subscapularis. When they work properly, you can rotate your arm, lift it overhead, and perform thousands of movements without thinking about it. When something goes wrong, you feel it immediately.
The rotator cuff is particularly vulnerable because it does so much work. It stabilizes the shoulder during movement, not just when you're lifting heavy things, but during everyday activities: reaching for your coffee mug, throwing a ball, pushing a door open, swimming, working overhead.
Over decades of use, these tendons develop changes. Microtears occur. Fibers fray. The tissue develops small defects. In the language of radiology, these become "abnormalities."
But here's where the disconnect happens. The radiologist describes these changes precisely because they're trained to report everything they see. That's their job. But "abnormal" in the imaging sense doesn't equal "abnormal" in the clinical sense—meaning it doesn't automatically mean something is wrong with how your shoulder functions.
This distinction is everything.
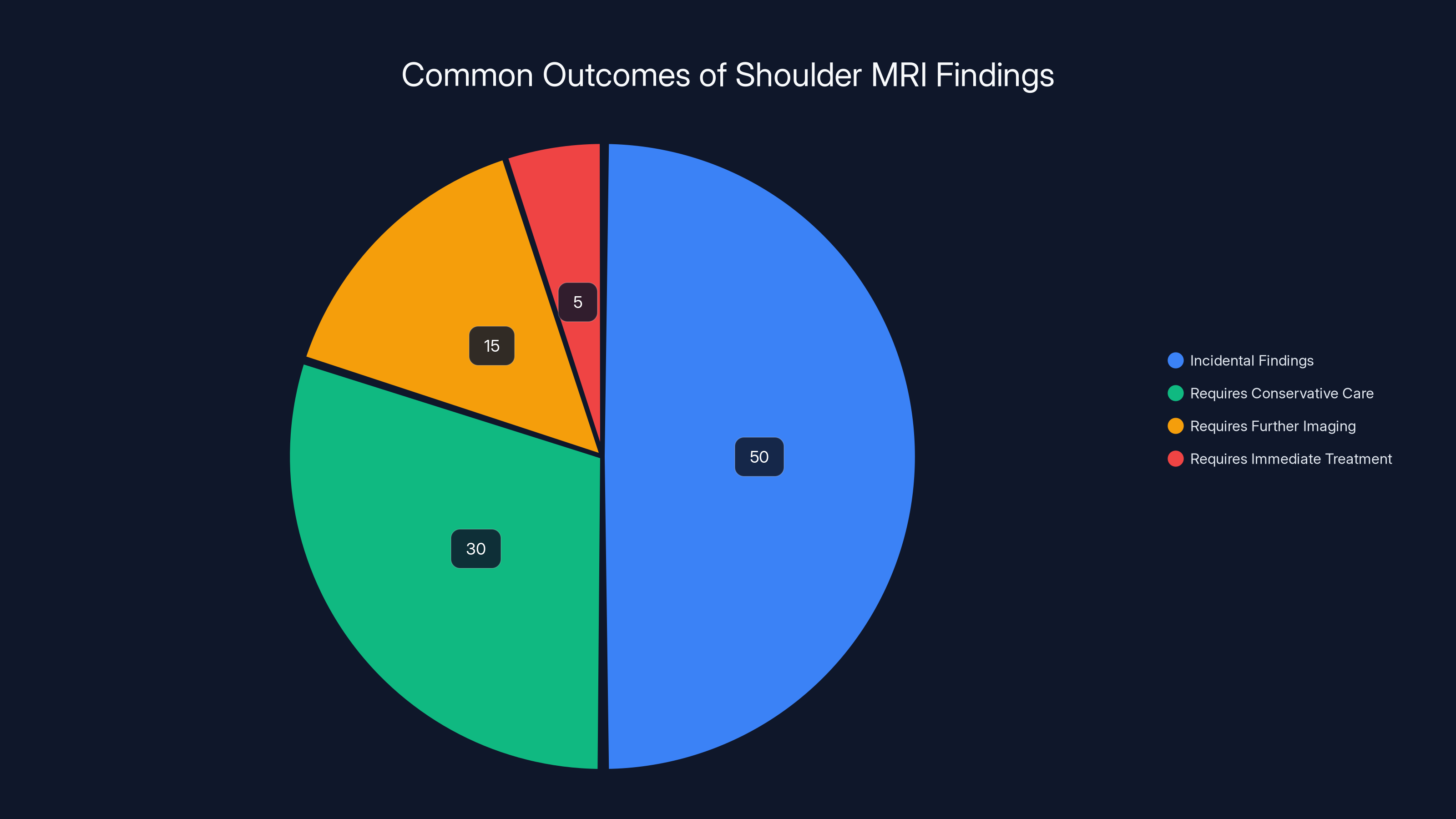
Estimated data shows that most shoulder MRI findings are incidental and do not require immediate treatment. Conservative care is often sufficient.
The Landmark Finnish Study: What Researchers Actually Found
Let's look at the numbers because they're striking.
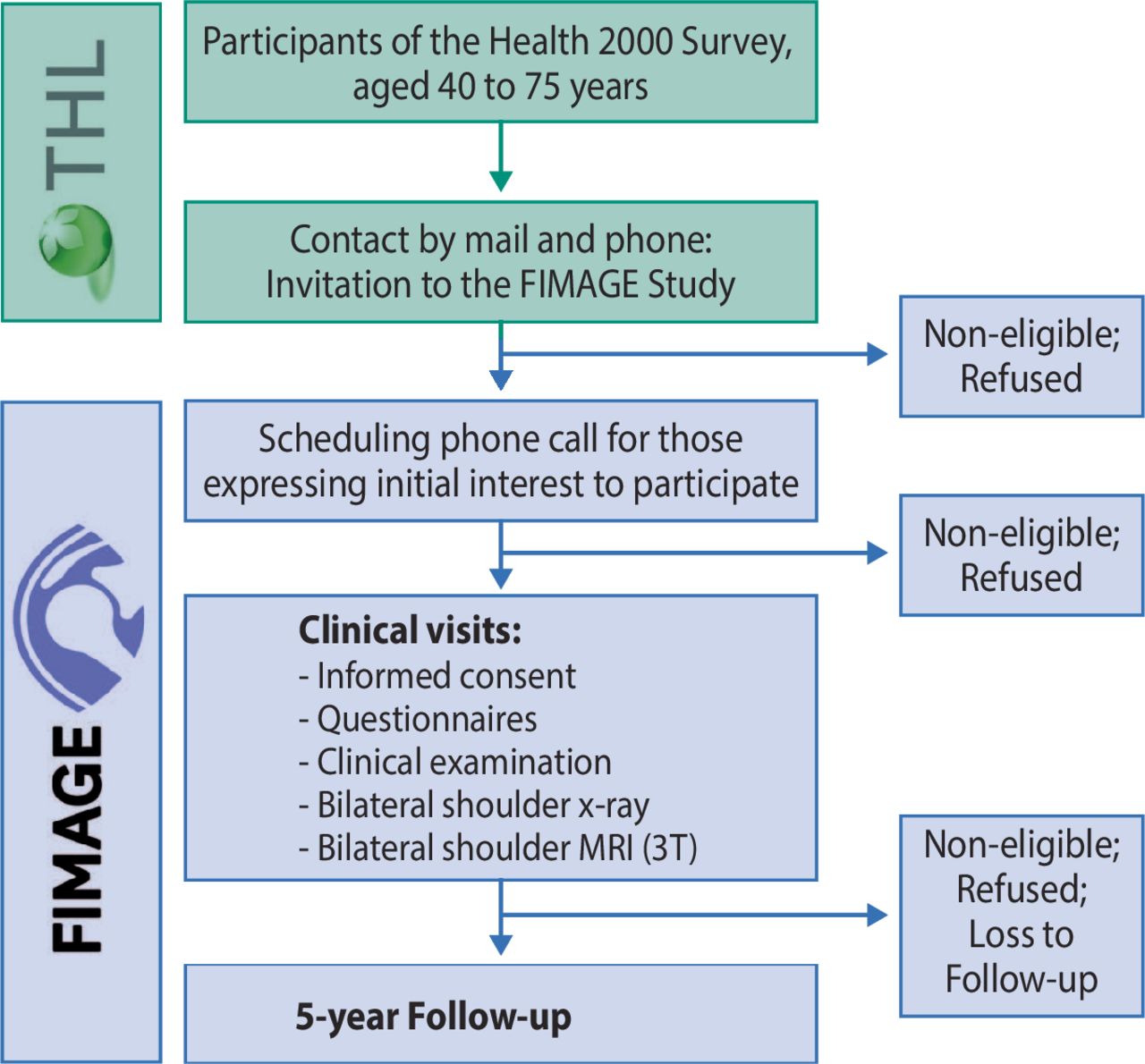
The study was conducted by Finnish researchers who accessed a nationally representative sample of adults participating in a public health survey. They recruited 602 participants (with one notable exception: they excluded anyone with previous shoulder surgery), aged 41 to 76, and performed bilateral shoulder MRIs on every single person.
Then they asked them questions: Do you have shoulder pain? If so, where? For how long? Does it interfere with your daily life?
Here's what they discovered:
Of the 602 people scanned:
Of the 1,204 individual shoulders analyzed (602 people × 2 shoulders):
Now for the abnormalities. The MRI revealed that 595 of the 602 people (98.8%, effectively 99%) had at least one rotator cuff abnormality. Here's the breakdown of what they found:
Most common findings:
- Partial-thickness tears: 62% of all participants
- Tendinopathy (tendon swelling/thickening): 25% of all participants
- Full-thickness tears: 11% of all participants
When researchers looked at the asymptomatic shoulders specifically (the 1,076 shoulders in people with no pain):
For symptomatic shoulders (the 128 with pain):
So the rate of abnormalities was nearly identical between pain and no pain groups.
When researchers looked more closely at specific types of abnormalities, something interesting happened. Full-thickness tears initially appeared more common in the symptomatic group. But when researchers adjusted their analysis for other confounding variables (like the presence of multiple additional abnormalities, age, body mass index), that difference essentially vanished.
In other words: even the most severe abnormality (full-thickness tear) didn't clearly correlate with whether someone had pain.
The Age Progression: Why Older Doesn't Always Mean Worse
One clear pattern did emerge: age-related progression.
Researchers found that abnormalities increased with age, but not uniformly.
Full-thickness tears, for instance, were completely absent in participants under 45 years old. But by ages 70 to 76, they were significantly more common. Partial-thickness tears and tendinopathy also increased with age.
But here's what's important: the presence of these age-related changes didn't correlate with the presence of pain. Older people had more abnormalities, but they weren't in more pain. The relationship between imaging findings and symptoms remained weak across all age groups.
This tells us something crucial: age-related structural changes are normal. They're expected. They're part of how human tissues change over time. Just like your skin changes with age, your tendons and rotator cuff change with age.
The problem is when we label these normal aging processes with pathological language like "tear" and "damage." We create a false narrative that normal is broken.
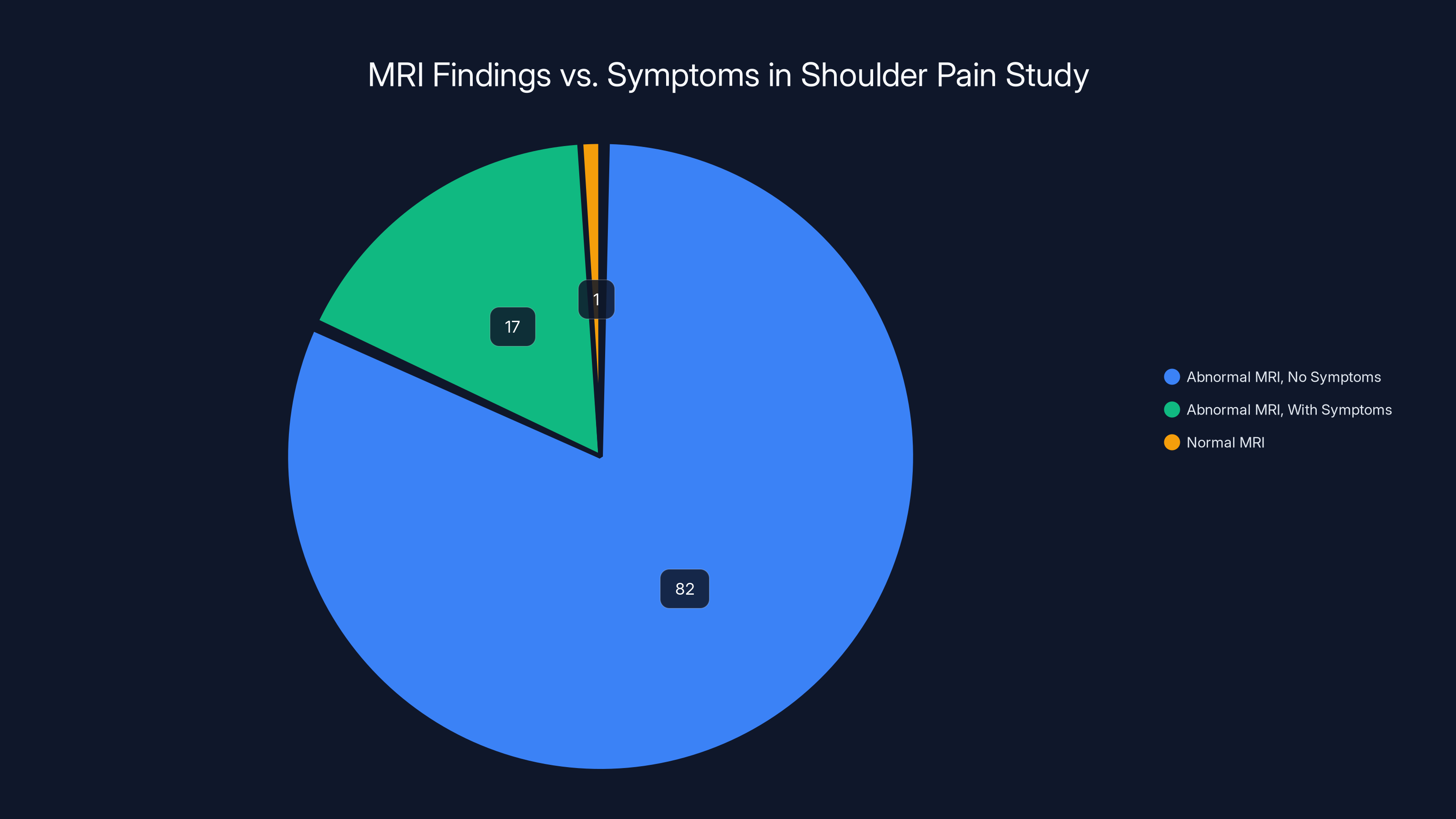
The study found that 82% of participants had abnormal MRI findings without any symptoms, highlighting a disconnect between MRI results and clinical symptoms in shoulder pain diagnosis.
The Gender Finding: No Meaningful Difference Between Men and Women
Researchers also broke down their findings by gender.
The prevalence of rotator cuff abnormalities was remarkably similar between males and females. Both groups showed the same rates of partial-thickness tears, tendinopathy, and full-thickness tears.
Both groups also showed the same weak correlation between imaging abnormalities and actual symptoms.
This is an important null finding. It tells us that rotator cuff changes aren't driven by sex-based hormonal factors or biomechanical differences that would affect men and women differently. Instead, they appear to be a universal feature of aging in humans.
The implication: if you're a woman over 40 getting an MRI, don't assume your results are different or more severe than what a man your age would experience. The prevalence is essentially identical.
Why MRI Abnormalities Don't Equal "You Need Surgery"
This is perhaps the most important takeaway.
MRI machines are incredibly good at their job. They can detect minute structural changes in soft tissue. They can show a partial-thickness tear that's just a few millimeters. They can reveal tendon fiber disruption that might not affect function at all.
But exquisite sensitivity in detecting structural changes does not equal clinical relevance.
A structural change only matters if it changes how your shoulder functions or causes pain. And this study clearly shows that the vast majority of MRI-detected abnormalities do exactly neither.
Yet here's what happens in clinical practice:
- Patient has shoulder pain or gets an MRI for some other reason
- MRI finds an "abnormality"
- Doctor shows patient the report and uses pathological language
- Patient becomes concerned
- Conversation shifts toward whether the patient "needs" treatment or surgery
- Patient anxiety escalates
- Unnecessary treatments or procedures follow
This cascade is documented extensively in orthopedic literature. Studies show that when patients are told they have a "tear" on imaging, they're far more likely to perceive pain, expect that pain will worsen, and pursue more aggressive treatment.
It's a self-fulfilling prophecy created by language.
The study authors put it plainly: "While we cannot dismiss the possibility that some RC tears may contribute to shoulder symptoms, our findings indicate that we are currently unable to distinguish clinically meaningful MRI abnormalities from incidental findings."
Translation: we can see the abnormalities, but we can't tell which ones actually matter.
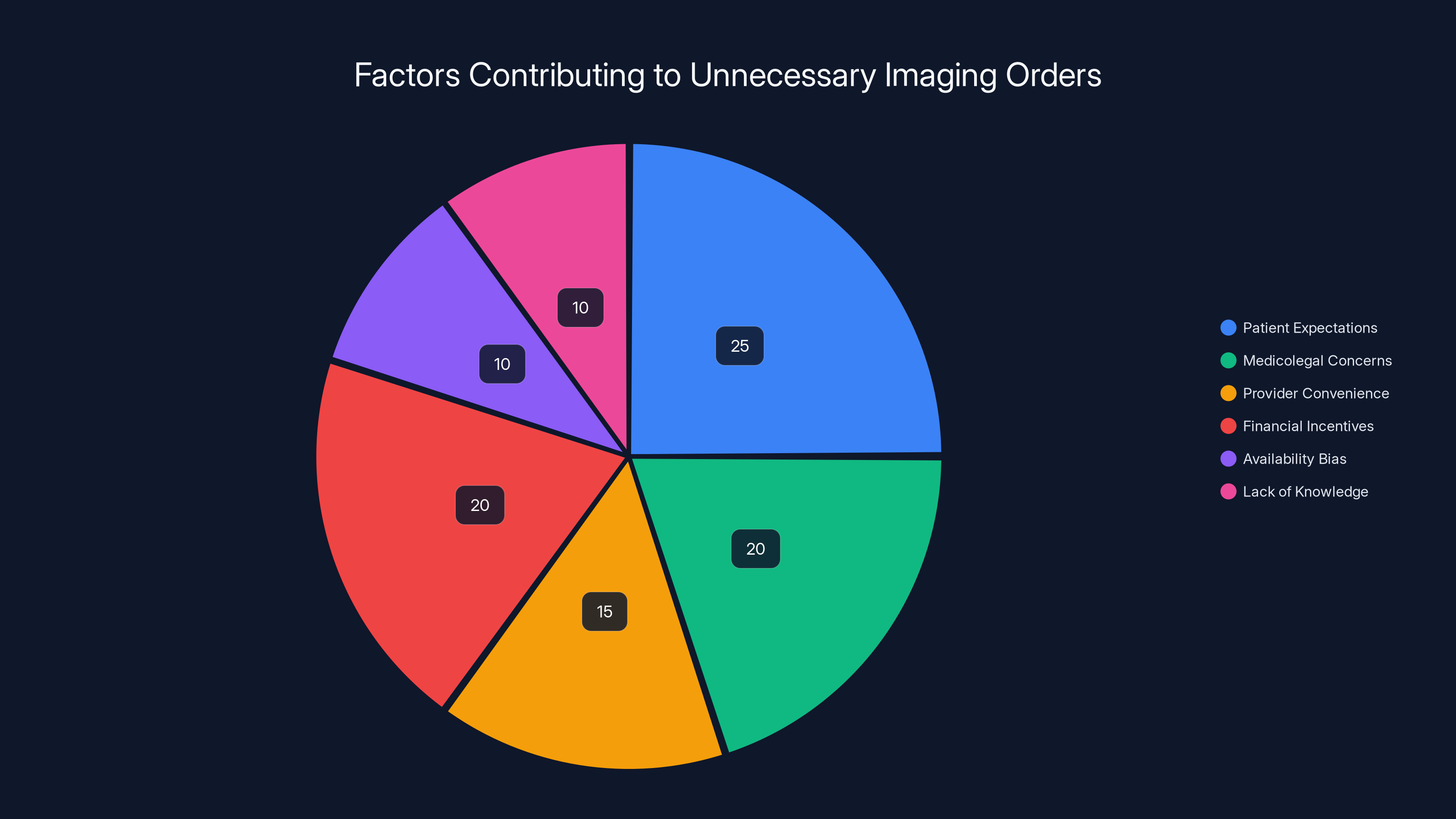
Patient expectations and financial incentives are major drivers of unnecessary imaging, each contributing to about 20-25% of cases. Estimated data.
The Language Problem: Why "Tear" Is the Wrong Word
The authors of the study make a compelling argument about terminology, and it's worth taking seriously.
When a radiologist reports a "tear" in your rotator cuff, you imagine damage. You imagine something ripped. You imagine urgency. You imagine repair.
But many of these "tears" are more accurately described as normal age-related structural changes. The tissue hasn't torn apart in the traumatic sense. Fibers have disrupted, edges have frayed, the tissue has developed small defects. These are predictable, expected changes that happen to nearly everyone over time.
Calling them "tears" implies a traumatic injury. It implies something went wrong that needs fixing.
The study authors propose using more precise, less value-laden terminology:
- Lesion (instead of tear)
- Defect (instead of tear)
- Fraying (describing exactly what's happening)
- Disruption (describing fiber separation)
- Structural alteration (describing what changed)
- Degeneration (describing age-related changes)
These words are more accurate and—critically—they don't trigger the same cascade of anxiety and treatment pursuit that "tear" does.
Language shapes perception. Perception shapes behavior. Behavior shapes outcomes.
If you're told you have a "rotator cuff lesion with some fraying," you're far more likely to respond differently than if you're told you have a "rotator cuff tear." Both could be describing the identical finding on the same MRI.

The Clinical Exam Problem: What Gets Overlooked
Here's what's frustrating about relying on MRI: the clinical exam gets downgraded in importance.
When a doctor suspects shoulder pain, they should do specific tests:
- Range of motion testing: Can you move your arm through normal ranges painlessly?
- Strength testing: Do specific muscles test weak?
- Provocative testing: Does the Neer test, Hawkins test, or empty can test reproduce your pain?
- Palpation: Where exactly does it hurt when the doctor presses on the shoulder?
- Functional assessment: Can you do the movements and activities that matter to you?
These tests tell you what's actually wrong with how the shoulder functions.
An MRI, by contrast, tells you what's structurally present. But presence and relevance are different things.
A good clinical exam can identify whether rotator cuff weakness exists and which specific muscles are involved. This information is far more clinically useful than knowing a partial-thickness tear is present.
Yet when an MRI is in the picture, it often becomes the dominant information source. Doctors organize their thinking around the imaging finding. The clinical exam becomes secondary confirmation rather than primary diagnostic tool.
The study authors and the orthopedic surgeons commenting on the study stress this repeatedly: diagnosis and management of shoulder pain should be guided primarily by functional limitations, clinical exam findings, and patient history—not by imaging results.

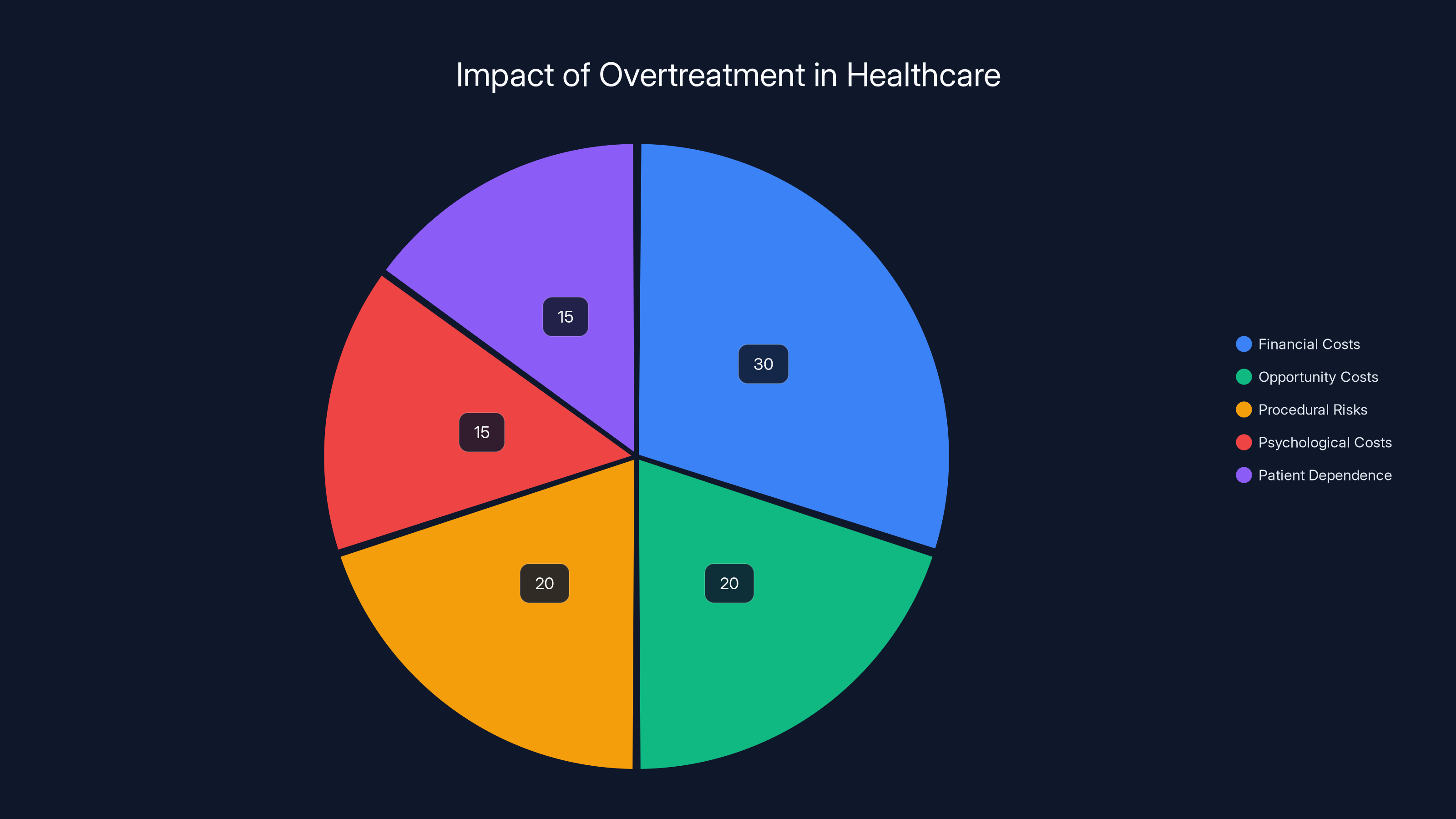
Estimated data shows financial costs as the largest consequence of overtreatment, followed by opportunity and procedural risks. Psychological costs and patient dependence also contribute significantly.
When MRI Actually Is Appropriate
The study findings don't mean MRI is useless for shoulder pain. Rather, they establish appropriate sequencing.
For non-traumatic shoulder pain (pain that developed gradually without a specific injury), the current evidence supports this approach:
First line: Conservative management (4-8 weeks)
- Rest and activity modification
- Physical therapy focused on strengthening and mobility
- Anti-inflammatory medications if appropriate
- Monitoring symptoms
If conservative care works: No MRI needed
- Many shoulder pain cases resolve or significantly improve with physical therapy alone
- If you're getting better, you don't need to know about incidental MRI findings
If conservative care doesn't work: Consider MRI
- After a trial of rest and physical therapy shows no meaningful improvement
- When you have persistent functional limitations
- When there's a specific question about whether imaging would change treatment decisions
For traumatic shoulder pain (pain following a specific injury like a fall or dislocation):
- MRI may be more appropriate earlier
- Imaging helps identify whether there's an actual structural injury requiring different treatment
- Trauma changes the calculus because you're looking for actual damage that happened acutely
The key principle: use MRI to answer a specific clinical question, not as a screening tool. Don't get an MRI just to see if something's wrong. Get an MRI when you have persistent symptoms despite appropriate conservative care and when the findings would actually change your treatment approach.
The Problem of Overtreatment: Why This Matters for Healthcare Costs
Overtreatment doesn't sound harmful. It sounds like "extra help."
But overtreatment has real consequences:
Financial costs: Unnecessary MRIs cost money. Unnecessary specialist consultations cost money. Unnecessary procedures cost money. In aggregate, inappropriate shoulder imaging and treatment cost the U. S. healthcare system billions annually.
Opportunity costs: A patient getting an unnecessary surgery for an asymptomatic MRI finding is a patient not getting physical therapy that might actually help. Time and resources are finite.
Procedural risks: Even minor procedures carry risks. Injections carry infection risk, allergic reaction risk, and risk of worsening symptoms. Surgery carries all those risks plus anesthesia risk and risk of causing new scar tissue. These risks only make sense if the benefit is clear.
Psychological costs: Being told you have a "tear" in your shoulder affects your self-perception. It affects your confidence. It affects your willingness to use that arm normally. These psychological effects can perpetuate or worsen pain and disability.
Creation of patient dependence: Once someone is in the surgical pathway, they're often in the surgical pathway. They're not trying physical therapy. They're not testing their own recovery potential. They're waiting for the next intervention.
The study's findings suggest these overtreatment scenarios are happening frequently. With 99% of adults over 40 having MRI abnormalities, yet only a small percentage having symptoms, the opportunity for inappropriate treatment is enormous.
If clinicians are recommending treatment based on imaging findings in asymptomatic patients, many of those treatments are unnecessary.
Estimated data shows that incidental findings are common across different imaging types, with abdominal CT scans having the highest percentage. Estimated data.
What the Orthopedic Surgeons Say: Clinical Wisdom From the Field
The study sparked an accompanying editorial from two respected orthopedic surgeons at the University of California, San Francisco: Edgar Garcia-Lopez and Brian Feeley.
Their perspective is worth noting because they're not anti-imaging and not anti-surgery. They're pro-appropriate-medicine.
They make several key points:
First, they endorse the language shift. Using less pathological terminology makes sense. It reduces unnecessary patient anxiety. It decreases the perception that something needs fixing simply because an abnormality exists.
Second, they emphasize the role of clinical context. The same MRI finding might mean very different things in different patients:
- A 45-year-old with acute trauma and weakness might need different management than a 65-year-old with gradual pain onset and preserved strength
- A competitive athlete with high functional demands might pursue different treatment than someone with recreational activity level
- A patient with significant functional limitation might choose treatment that someone with minimal limitations would reasonably decline
Third, they establish appropriate sequencing for non-traumatic shoulder pain:
-
Watchful waiting with conservative care first (weeks to couple months)
- This alone resolves many cases
- Patients regain confidence and function
- No risk from intervention
-
Only proceed to MRI if conservative care fails and symptoms persist
- At that point, imaging might clarify what's happening
- But even then, imaging should guide treatment selection, not mandate treatment
-
Base treatment decisions on clinical exam and functional limitations, not imaging findings
- This is perhaps the most important principle
- The patient's ability to move and function matters more than what the MRI shows
Fourth, they distinguish when MRI is most useful:
- When you suspect a specific structural problem that would change treatment (like a rotator cuff tear that might benefit from surgery)
- When there's persistent pain despite conservative care and you want to understand why
- After trauma when you're evaluating actual structural damage
What they don't recommend is using MRI as a screening tool or ordering it routinely for shoulder pain.

Physical Therapy: The Evidence for Non-Surgical Management
If MRI abnormalities don't automatically require treatment, what does work for shoulder pain?
The evidence strongly supports physical therapy as first-line treatment.
Multiple large studies show that structured physical therapy—focusing on rotator cuff strengthening, scapular stabilization, posture correction, and mobility work—resolves most cases of shoulder pain, even cases with MRI-documented structural abnormalities.
Here's what effective physical therapy typically includes:
Phase 1: Pain management and mobility (weeks 1-2)
- Gentle passive range of motion
- Modalities like ice or heat as needed
- Identifying and modifying movements that worsen pain
- Patient education about the condition and expectations
Phase 2: Strengthening initiation (weeks 3-4)
- Isometric strengthening (muscles contract without moving)
- Beginning to strengthen the rotator cuff
- Beginning scapular stabilization work
- Gradual increase in active range of motion
Phase 3: Progressive strengthening (weeks 5-8)
- Advancing to isotonic exercises (muscles contract while moving)
- Increasing resistance and repetitions
- Sport-specific or activity-specific exercises
- Improving functional movement patterns
Phase 4: Return to function (weeks 9-12)
- Advancing to dynamic stabilization
- Activity-specific training
- Return to sport or demanding activities
- Long-term maintenance program
Studies show that this approach is effective even for patients with confirmed rotator cuff tears. The strengthening of supporting muscles, improvement in scapular mechanics, and restoration of normal movement patterns often allow people to return to full function despite structural abnormalities.
The key requirement: consistency and appropriate progression. You can't do a couple of physical therapy sessions and expect results. Physical therapy requires patient participation and commitment over weeks and months.
Red Flags: When MRI and Specialist Consultation Actually Are Needed
We've established that most shoulder pain doesn't require MRI. But some situations are different.
Seek imaging or specialist consultation if you have:
Acute trauma with immediate weakness
- Fell on your shoulder and immediately lost strength
- This suggests possible acute rotator cuff tear
- MRI can help identify whether surgery might be appropriate
Progressive neurological symptoms
- Numbness or tingling that's getting worse
- Suggests possible nerve involvement
- Imaging might identify compression or other structural issues
Severe night pain unrelieved by conservative care
- Pain so severe it prevents sleep despite weeks of physical therapy
- Severe pain sometimes indicates more significant structural problems
- Worth investigating with imaging
Profound weakness that doesn't improve
- Unable to lift your arm overhead despite months of physical therapy
- Suggests possibly significant muscular or nerve problems
- Imaging might clarify what's happening
Signs of infection
- Fever, increasing warmth, spreading redness
- Suggests possible infection rather than mechanical problem
- Requires different evaluation and treatment
Failure to improve after 8-12 weeks of appropriate physical therapy
- If you've done consistent, structured physical therapy and haven't improved at all
- That's a reasonable point to get imaging to understand what might be limiting improvement
- But even then, imaging guides treatment, not mandates it
Absent these red flags, conservative management should be the starting point.
The Economics of Imaging: Why Inappropriate Ordering Happens
If MRI for every shoulder pain complaint doesn't make sense clinically, why is it so commonly ordered?
Several factors drive unnecessary imaging:
Patient expectations
- Patients often expect imaging to be part of diagnosis
- "We need to get a picture of what's going on" feels right to patients
- Physicians feel pressured to order imaging to meet patient expectations
- Ordering an MRI is often easier than explaining why it's not needed yet
Medicolegal concerns
- Doctors worry about missing something
- "I ordered an MRI" creates a paper trail showing they investigated
- Not ordering an MRI is harder to defend later if something goes wrong
- This defensive medicine drives unnecessary imaging
Convenience for the provider
- Ordering an MRI is quick
- It shifts responsibility to the radiologist (who interprets it) and specialist (who decides treatment)
- It avoids having a longer conversation about conservative management
Financial incentives
- In some healthcare systems, ordering more imaging generates more revenue
- Procedures and imaging are often reimbursed better than conservative management
- Some practices benefit financially from ordering more imaging
Availability bias
- If you work somewhere where MRI is readily available, you tend to order it more
- If it requires jumping through hoops to get MRI, it's ordered more selectively
Lack of knowledge about base rates
- Many clinicians aren't aware that 99% of asymptomatic adults over 40 have MRI abnormalities
- If clinicians think abnormalities are uncommon, finding one seems significant
- Understanding the base rate changes how you interpret findings
Addressing overimaging requires changing incentives, education, and expectations. It requires patients understanding that not all abnormalities need treatment. It requires doctors comfortable saying "let's try conservative care first." It requires healthcare systems rewarding appropriate diagnosis rather than procedural volume.
How to Interpret Your Own Shoulder MRI Report
If you've already gotten an MRI, here's how to think about your results without panic.
What the report might say and what it actually means:
"Rotator cuff tear"
- This might be a full-thickness tear (tendon completely severed)
- More commonly, it's a partial-thickness tear (tendon partially disrupted)
- Or it might just be some fraying/disruption
- Presence of a tear doesn't automatically mean you need surgery or treatment
- Context matters: Are you in pain? Is your strength normal? Can you do your activities?
"Tendinopathy" or "tendinosis"
- This means the tendon shows signs of inflammation or degeneration
- It's very common in people over 40
- By itself, it doesn't require treatment
- Many people have tendinopathy with zero symptoms
"Subacromial spurring"
- This is bone spur formation near the rotator cuff
- Common with age
- Doesn't automatically cause problems
- Only problematic if it's compressing tissue and causing pain
"Labral tear"
- The labrum is cartilage that lines the shoulder socket
- Labral tears are common findings
- Many are asymptomatic
- Some labral tears contribute to instability or catching
- Presence doesn't automatically require treatment
"Rotator cuff atrophy"
- The muscle looks smaller or less defined
- Can indicate long-standing problems or disuse
- Doesn't automatically mean current strength is reduced
- Should be correlated with actual strength testing
"Mild degenerative changes"
- This is a polite way of saying "age-related changes"
- Expected in adults over 40
- Not necessarily problematic
- Doesn't automatically require treatment
When you get your report:
- Ask your doctor: Does this finding explain your pain?
- Ask your doctor: Would treatment change based on this finding?
- Ask your doctor: Is this something we need to treat or something we can monitor?
- Ask your doctor: What would happen if we didn't treat this?
If your doctor can't clearly explain why this finding changes treatment, that's important information. It suggests the finding might be incidental.

The Future of Shoulder Imaging: Moving Toward Appropriate Care
The Finnish study is driving important conversations about how shoulder imaging should be used.
Experts are moving toward criteria-based imaging. In other words, imaging should have clear indications. You image when you suspect something specific that would change management, not to screen for possible problems.
Some healthcare systems are implementing imaging guidelines that encourage:
- Trial of conservative care first before imaging for non-traumatic pain
- Clear documentation of what clinical question the imaging is meant to answer
- Specific findings that would change treatment identified before imaging is ordered
- Shared decision-making about what to do with findings once they're identified
This approach has multiple benefits:
- Reduced costs: Fewer unnecessary imaging studies
- Better patient outcomes: Fewer unnecessary treatments
- Reduced anxiety: Fewer incidental findings creating worry
- More time for proven therapies: Physical therapy gets more emphasis
The conversation is also shifting around what terminology radiologists use. Some systems are moving toward language that's less pathological and more descriptive, aligned with what the study authors recommended.
Over the next few years, we'll likely see more shoulder pain cases managed conservatively first, with imaging used more selectively. This shift should improve outcomes while reducing healthcare costs.
What You Should Do If You Have Shoulder Pain
Let's make this practical.
If you have shoulder pain without recent trauma:
-
Start with conservative management
- Rest from activities that worsen it
- Ice if there's inflammation
- Basic stretching and gentle movement
- Activity modification
-
Consider physical therapy
- Find a PT experienced with shoulder pain
- Commit to 4-6 weeks of consistent sessions
- Do home exercises as prescribed
- Track your progress
-
Consider medication if needed
- Over-the-counter NSAIDs might help with inflammation
- Discuss with your doctor if appropriate for you
-
Be patient
- Shoulder pain often takes weeks to improve
- Expect gradual improvement, not immediate relief
- Consistency matters more than intensity
-
Get imaging only if
- You've tried conservative care for 4-8 weeks without improvement
- Your symptoms are severe and significantly limiting
- You want imaging to help guide treatment decisions
-
When you get imaging results
- Ask what they mean in plain language
- Ask if findings explain your pain
- Ask if findings would change your treatment
- Don't assume "abnormality" means "needs surgery"
-
Make treatment decisions based on function
- Can you do activities that matter to you?
- Is pain limiting you?
- These questions matter more than imaging findings
If you have shoulder pain after trauma:
-
Seek prompt evaluation
- Significant trauma might cause actual structural damage
- Evaluation might indicate need for imaging or specialist consultation
- But even then, conservative management is often first-line
-
Imaging might be appropriate earlier
- If you have immediate weakness after trauma
- If you have severe acute pain
- If you have numbness or neurological symptoms
-
Still prioritize conservative management
- Even with confirmed structural tears, many people do well with physical therapy
- Surgery isn't always necessary even with structural damage

The Bigger Picture: When Imaging Becomes a Problem
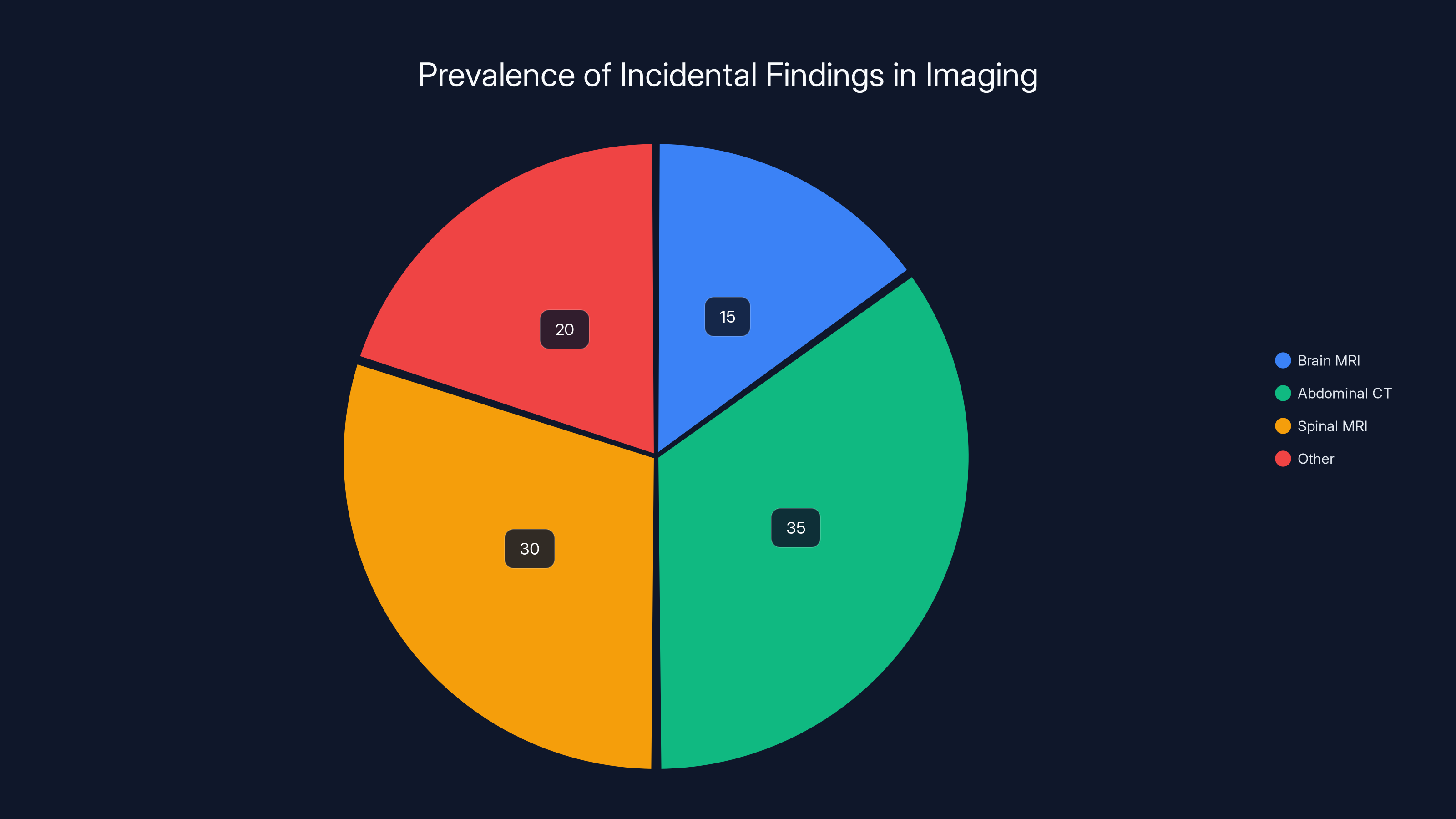
The shoulder MRI study is part of a much larger issue in healthcare: incidentalomas—findings on imaging that weren't the reason you got the imaging, and might not matter.
It's not just shoulders. Studies of brain MRI find incidental brain tumors in 1-2% of scans done for other reasons. Studies of abdominal CT find incidental findings requiring further investigation in a significant percentage of scans. Spinal MRI frequently shows disc bulges and degenerative changes unrelated to why someone got imaged.
Each finding triggers anxiety. Each one creates a cascade of follow-up tests, additional imaging, specialist consultations, and potential treatments.
Sometimes these findings are important. Sometimes they're red herrings that distract from the actual problem and drive unnecessary care.
The solution isn't avoiding imaging entirely. The solution is using imaging more thoughtfully: asking specific questions before imaging, being clear about what would change management, and understanding base rates of findings in asymptomatic populations.
The shoulder study provides a perfect case study of how to handle this problem correctly: identify which findings matter clinically, separate them from incidental changes, and base treatment on function rather than imaging.
FAQ
What does it mean if my MRI shows a rotator cuff tear but I have no pain?
It likely means you have a structural change that's not affecting your function. Research shows that the vast majority of MRI-detected rotator cuff abnormalities exist in people with no symptoms. If you're not in pain and your shoulder works normally, the finding is probably incidental. However, talk with your doctor about whether monitoring is appropriate or whether this changes any treatment decisions. The fact that you don't have symptoms is actually the most important information.
Should I get an MRI if I have shoulder pain?
Not necessarily right away. Current evidence suggests trying conservative management first: rest, physical therapy, activity modification, and time. If you've tried conservative care for 4-8 weeks without improvement and your pain is significantly limiting your activities, then MRI becomes more reasonable. An MRI is most useful when you have persistent symptoms despite conservative care and when the findings would actually change your treatment approach. Routine imaging for shoulder pain without preceding conservative care often leads to unnecessary findings and overtreatment.
How long should I try physical therapy before getting an MRI for shoulder pain?
The research suggests at least 4-8 weeks of consistent physical therapy before considering imaging for non-traumatic shoulder pain. This timeframe is enough for many shoulder conditions to improve or resolve. If you're showing meaningful improvement, you might not need imaging at all. If you've done consistent, structured physical therapy with a qualified therapist and haven't improved at all, that's a reasonable point to discuss imaging with your doctor. The key is consistency: you need to actually do the exercises and attend sessions regularly for this timeline to be meaningful.
Can you have a rotator cuff tear and still use your shoulder normally?
Yes, absolutely. This is one of the most important findings from the MRI research. Many people with documented rotator cuff tears have normal strength, normal range of motion, and no pain. They can lift their arm, carry objects, and do all normal activities. The body compensates. Other muscles take over. Many tears don't progress or cause problems. A structural tear on imaging doesn't automatically mean your shoulder won't function normally or that you'll develop pain.
What language should my doctor use when explaining MRI findings?
Descriptive language is better than pathological language. Instead of "tear," your doctor should describe what's actually present: partial disruption of the tendon, fraying at the edges, tendon thinning, or structural alteration. Instead of "abnormality," your doctor might describe "age-related changes" or specific structural findings. The language your doctor uses affects how you perceive your shoulder and whether you think it needs treatment. If your doctor uses alarming language, ask them to clarify exactly what's present and whether this finding explains your symptoms.
Do I need surgery for a rotator cuff tear I can see on MRI?
Not necessarily. The decision to pursue surgery should be based on whether the tear is causing symptoms and functional limitation, not simply on whether it exists. Many people with rotator cuff tears do well with conservative management, physical therapy, and maintaining activity. Surgery becomes more appropriate if you have persistent weakness despite conservative care, if symptoms significantly limit activities you care about, or if you have traumatic tears with significant symptoms. The presence of a tear on MRI alone doesn't automatically indicate surgery is needed.
What percentage of shoulder pain is actually caused by rotator cuff tears?
This is harder to answer than it seems because many people with tears have no pain. Among people who do have shoulder pain, rotator cuff tears account for a portion, but probably not as large a portion as MRI findings suggest. Many people with shoulder pain have normal rotator cuff anatomy. Many people with rotator cuff tears on imaging have no pain. This mismatch is exactly why the Finnish study was so important: it shows we can't assume an MRI finding explains the pain.
How do I find a physical therapist who specializes in shoulder pain?
Look for therapists with specific shoulder experience and credentials. Ask whether they have experience treating rotator cuff pain, rotator cuff tears, and non-surgical shoulder rehabilitation. Ask about their approach to strengthening versus stretching. Ask whether they use evidence-based protocols. Good shoulder specialists focus on progressive strengthening, scapular stabilization, and functional movement. They should also assess your posture, your mechanics, and movement patterns, not just isolated muscles. If your pain isn't improving after 2-3 weeks with a therapist, consider seeking a second opinion from another qualified therapist.
Key Takeaways on Shoulder MRI and Diagnosis
The Finnish study and its implications change how we should think about shoulder pain and imaging:
-
Structural findings on MRI don't automatically equal clinical problems that need treatment. Asymptomatic abnormalities are incidental findings that should rarely drive treatment decisions.
-
Language shapes perception and behavior. Calling age-related changes "tears" increases patient anxiety and drives unnecessary treatment. More precise terminology helps patients understand their condition accurately.
-
Conservative care should be first-line for non-traumatic shoulder pain. Physical therapy, rest, and activity modification resolve most cases. Imaging should come later if conservative care fails, not before it's tried.
-
Clinical exam and functional assessment matter more than imaging. Whether your shoulder works normally and whether you can do activities that matter to you are the most important diagnostic questions. MRI findings are supporting information, not primary diagnosis.
-
Base rate matters. When you understand that 99% of asymptomatic adults over 40 have MRI abnormalities, an incidental finding becomes far less concerning. It's normal, not unusual.
-
Age-related structural changes are expected and normal. We don't treat all of them. We monitor, support with physical therapy, and only pursue more aggressive treatment if symptoms warrant it.
-
Overtreatment has real costs: financial, physical (procedural risks), and psychological (anxiety from scary language). Judicious use of imaging helps prevent overtreatment.
If you're dealing with shoulder pain, remember that most cases resolve with conservative management. If you've already gotten an MRI showing "abnormalities," remember that most of these don't need treatment. And if you're considering shoulder imaging, ask yourself whether the findings would actually change how you're managing your pain. If the answer is no, you might not need the imaging.
The science is clear: normal anatomy doesn't require treatment just because an MRI shows it. What matters is function, symptoms, and whether an intervention would meaningfully improve your life. The Finnish study gives us permission to think about shoulder pain—and much of modern healthcare—quite differently.