![Guinea Worm Eradication: The Race to Eliminate Humanity's Second Disease [2025]](https://tryrunable.com/blog/guinea-worm-eradication-the-race-to-eliminate-humanity-s-sec/image-1-1770057978389.jpg)
Introduction: The Silent Victory Nobody's Talking About
Imagine a disease so painful that infected people voluntarily plunge their limbs into water just to numb the agony. Now imagine that disease has gone from affecting 3.5 million people in 1986 to just 10 cases in 2025. That's the Guinea worm eradication story, and it's one of the most remarkable public health achievements of our time, yet most people have never heard of it.
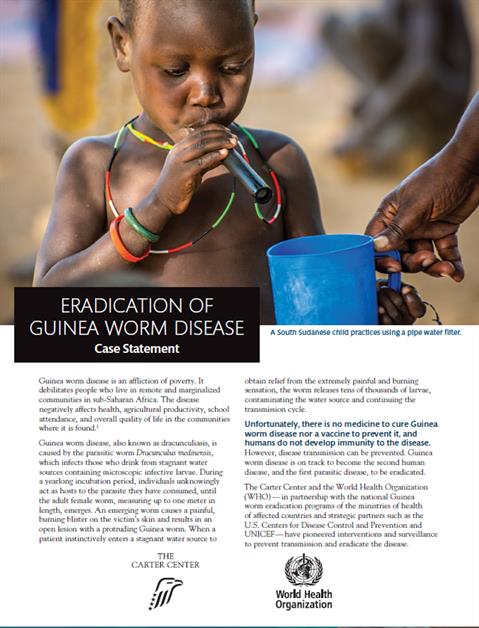
Guinea worm disease (dracunculiasis) caused by the parasitic nematode Dracunculus medinensis isn't a flashy disease. It doesn't kill quickly like smallpox or spread explosively like COVID-19. Instead, it's a slow, methodical torturer. The worm lives inside you, grows to the length of a cooked spaghetti noodle, and then emerges through your skin in an excruciatingly painful blister that can take two months to fully discharge. But that's exactly why its near-eradication is so impressive. Success wasn't achieved through a vaccine or a miracle drug. It was achieved through persistence, infrastructure, community engagement, and a commitment that spans four decades.
The Carter Center announced in early 2026 that 2025 saw only 10 confirmed human cases of Guinea worm globally. That's provisional until official confirmation in April, but if it holds, we're witnessing the death of a disease that once crippled millions. Only smallpox has been fully eradicated from human populations. Polio remains tantalizingly close but hasn't crossed the finish line. Guinea worm is about to.
But here's what makes this even more compelling: this isn't a story about cutting-edge biotechnology or billion-dollar pharmaceutical companies. It's a story about problem-solving with the tools you have. It's about cash incentives for reporting cases. It's about teaching people to boil water. It's about following every single lead, knowing each case represents a real person you can save from permanent disability. In an era where we're constantly chasing the next breakthrough, Guinea worm eradication reminds us that sometimes the greatest victories come from doing simple things relentlessly well.
TL; DR
- Only 10 human cases reported in 2025: Down from 3.5 million in 1986, Guinea worm is on track to become the second eradicated human disease
- Smallpox remains the only eradicated disease: Guinea worm's eradication would represent a historic public health milestone
- Four decades of sustained effort: The eradication campaign has prevented an estimated 100 million cases since 1986
- Simple interventions work: Water boiling, filtration, filtration cloth distribution, and cash rewards have been more effective than waiting for a vaccine
- Animal reservoirs complicate final elimination: While human cases near zero, animal infections in cattle and dogs require parallel eradication efforts
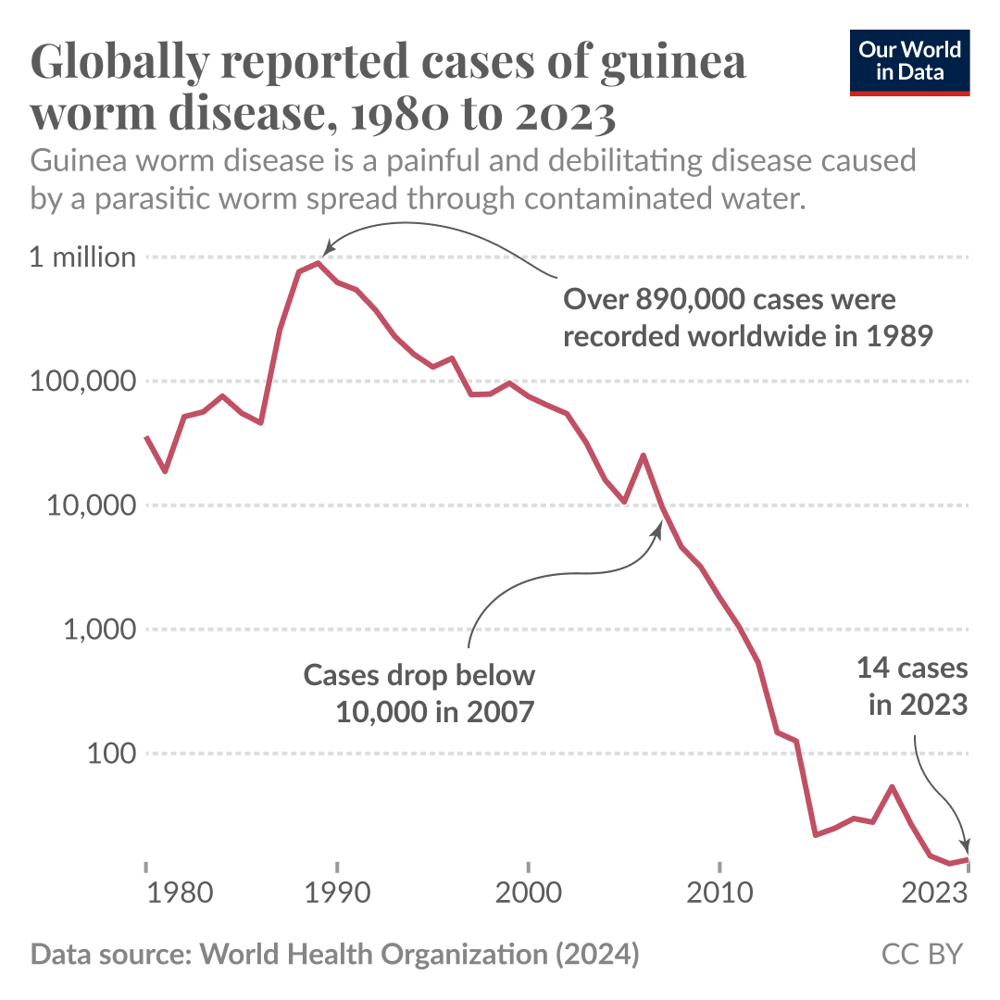
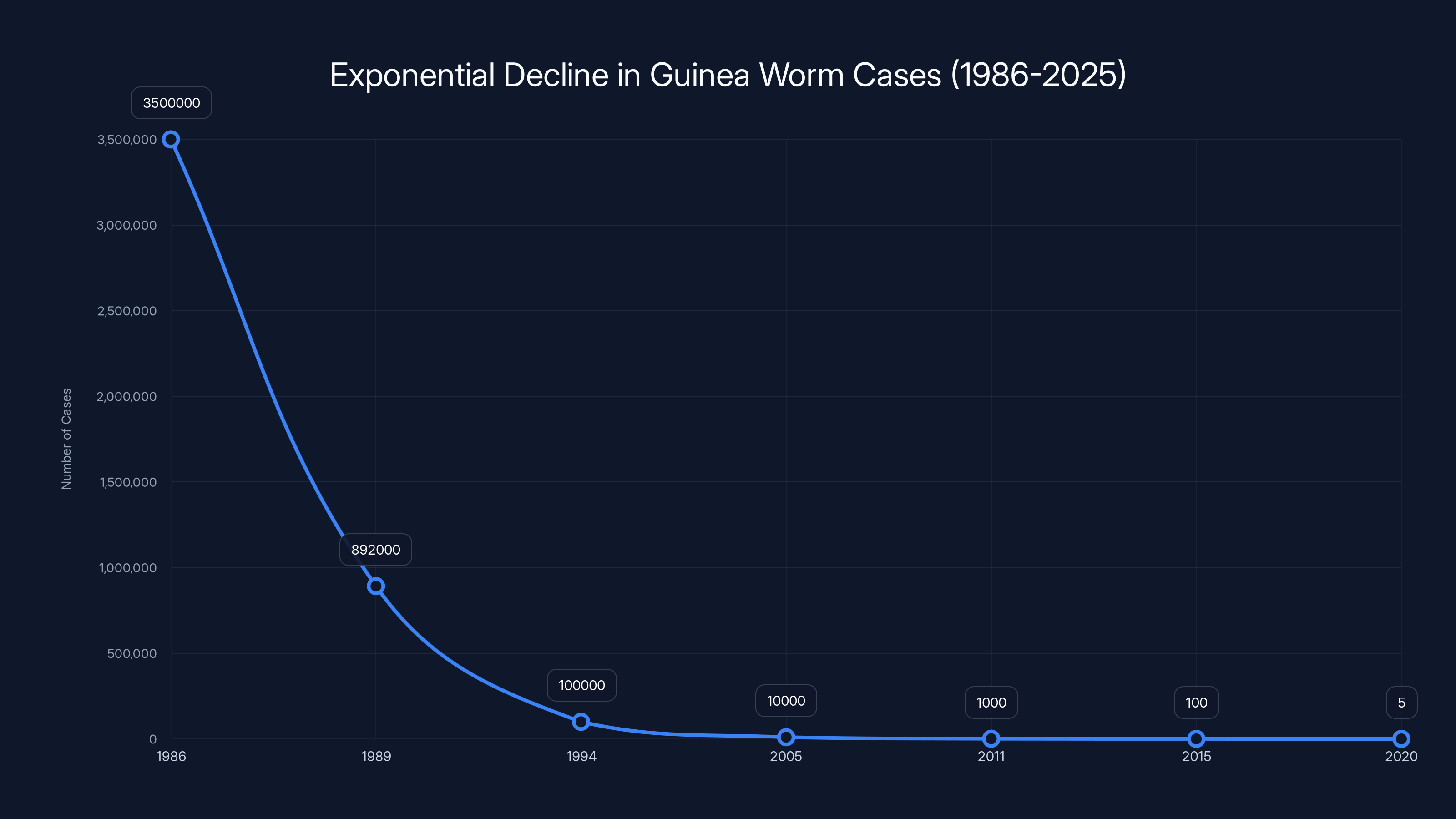
The chart illustrates the exponential decline in Guinea worm cases from 3.5 million in 1986 to single digits by the early 2020s, highlighting the effectiveness of eradication efforts. Estimated data.
The Biology of Suffering: How Guinea Worm Infects and Damages
The Lifecycle Nobody Wants to Know About
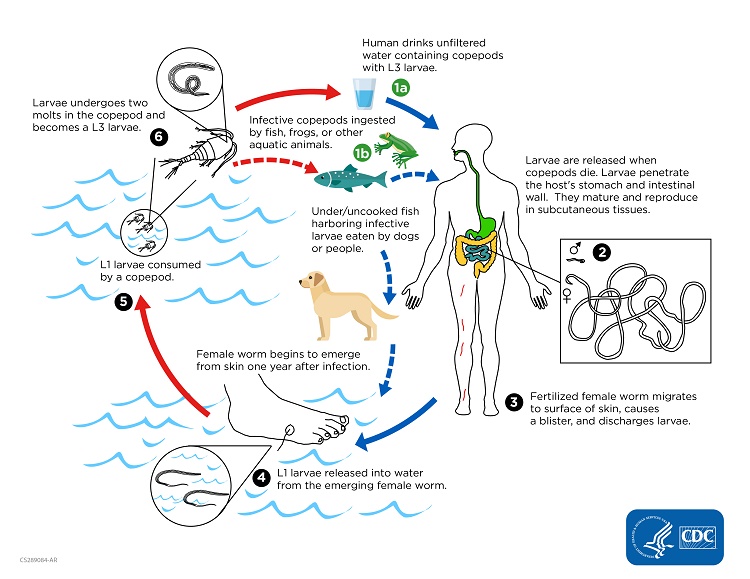
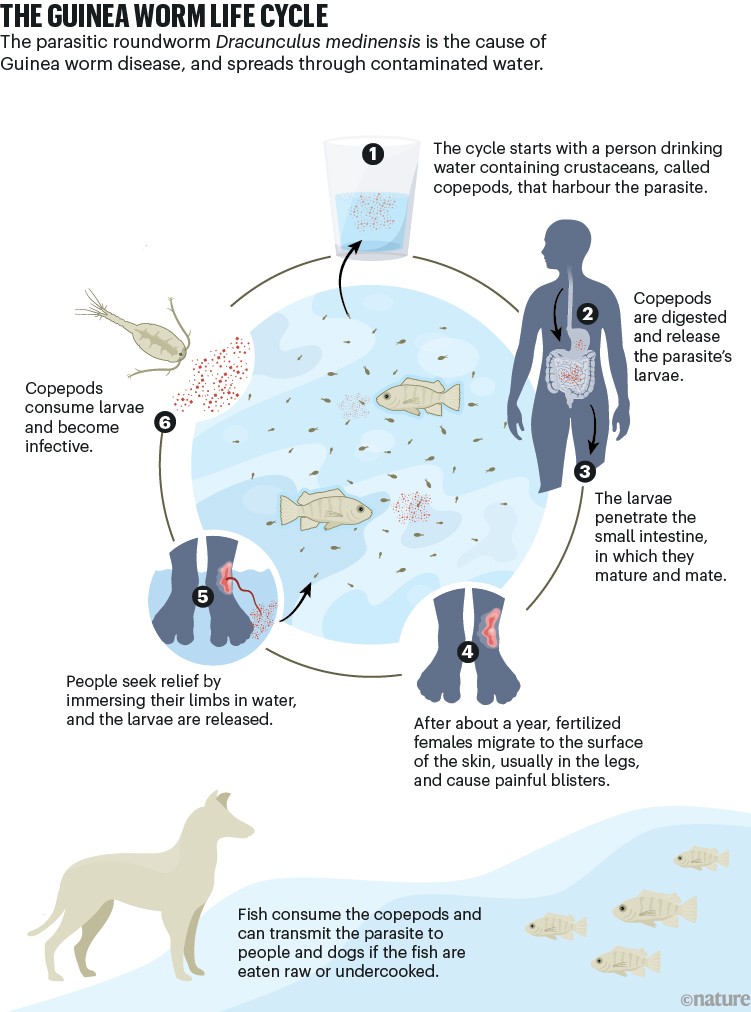
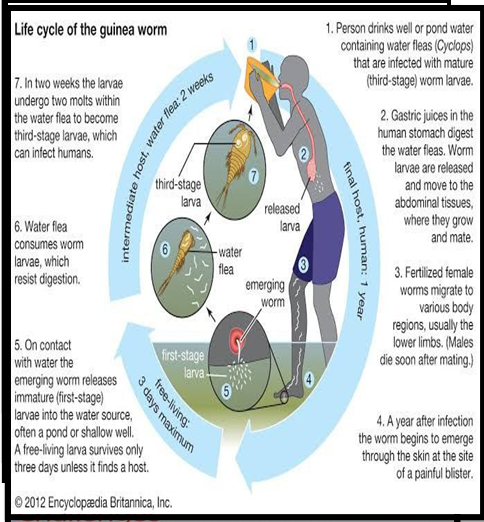
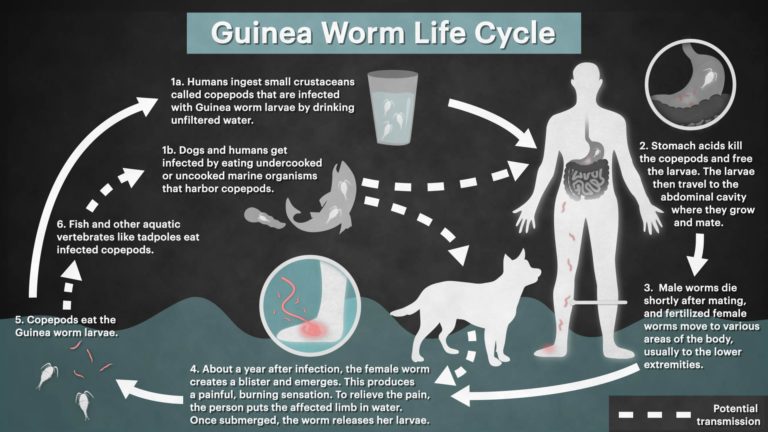
Understanding Guinea worm means understanding a lifecycle that sounds like it was designed by someone with a specific vendetta against human comfort. It starts innocuously enough: you drink contaminated water. That water contains tiny crustaceans called copepods, and those copepods are harboring Guinea worm larvae. You can't see them. You can't taste them. The water might even taste fine.
Once swallowed, the larvae begin their journey. They burrow through your intestinal tract with microscopic ruthlessness. Then they migrate through your abdominal cavity, moving through tissues with disturbing determination. This migration phase can last weeks, and you might not even notice anything wrong. Some people report mild symptoms like diarrhea or abdominal discomfort, but many have zero indication that a parasitic worm is setting up permanent residence.
Then comes year two. A blister forms, usually on your legs or feet, sometimes on your arms or torso. Inside that blister? The adult worm, now fully grown to somewhere between 60 centimeters and a meter in length. The blister ruptures, and the pain becomes the dominant feature of your existence. We're talking about pain so severe that people stop eating, stop working, stop functioning. One infected person becomes a household liability.
Here's the cruel mechanism that perpetuates transmission: the pain is so severe that people seek water to soak the affected limb. And when they do, the worm senses the temperature change and releases hundreds of thousands of larvae into the water. Someone else drinks that water. The cycle continues. Evolution didn't design this parasite to be considerate.
The Spectrum of Complications
Beyond the immediate pain, Guinea worm can trigger a cascade of devastating complications. Secondary bacterial infections are common because the open blister is essentially a wound gateway for any microbe in the environment. In areas without antibiotics, these infections can progress to sepsis, which can be fatal. Some patients develop tetanus if the wound isn't properly managed. The immobilization caused by the pain can lead to pressure ulcers and tissue death.
Most terrifying is the permanent disability aspect. If the worm emerges near a joint, it can cause chronic contractures where the joint permanently locks. People who were farmers, herders, or laborers become unable to work. In subsistence economies, disability often means poverty. It means your family goes hungry. Some villages had infection rates so high that entire communities couldn't function during Guinea worm season.
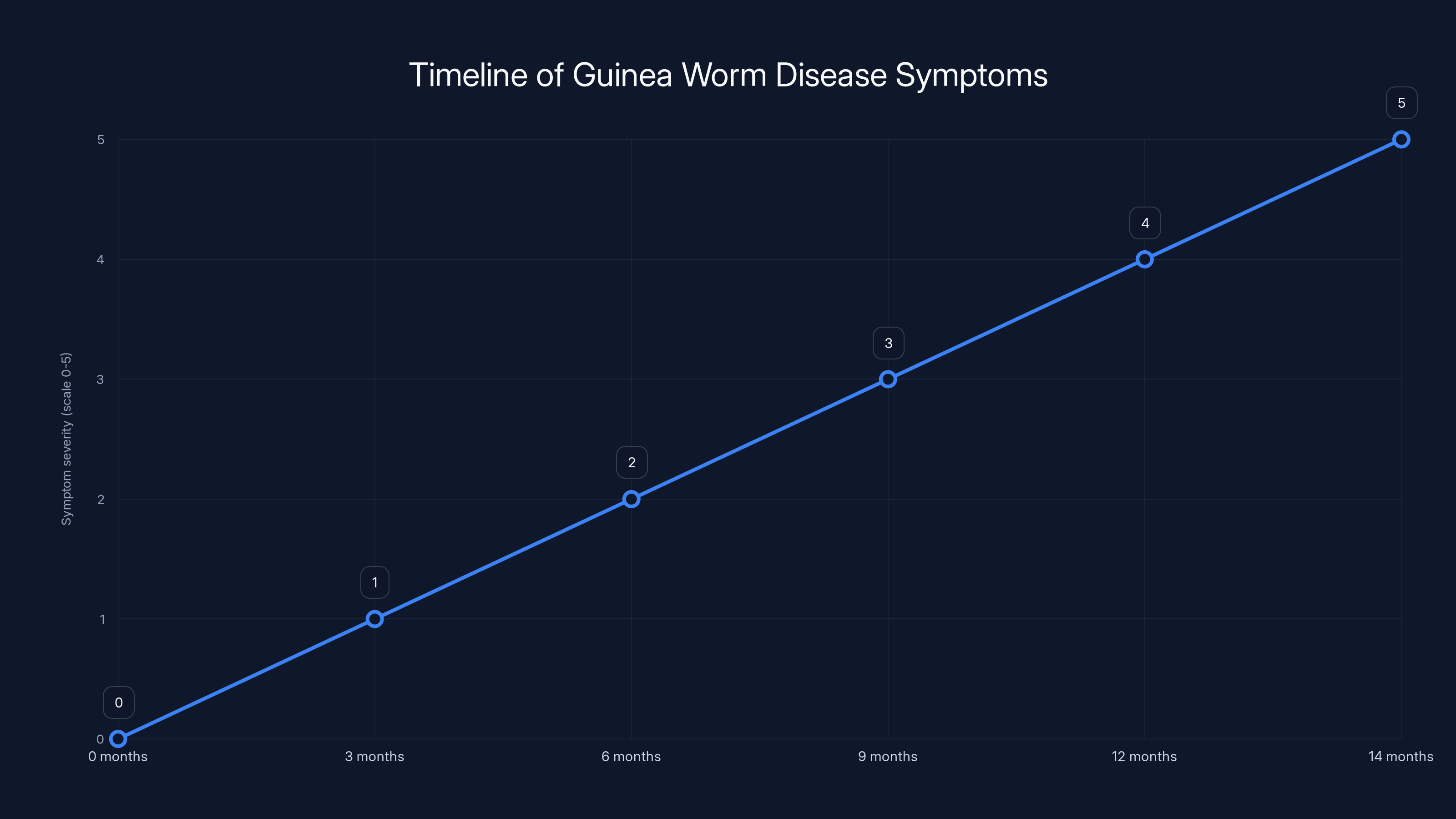
Estimated data shows that symptom severity increases gradually, peaking when the adult worm emerges 12-14 months post-infection.
The Global Footprint: Where Guinea Worm Still Exists
The Remaining Hotspots in 2025
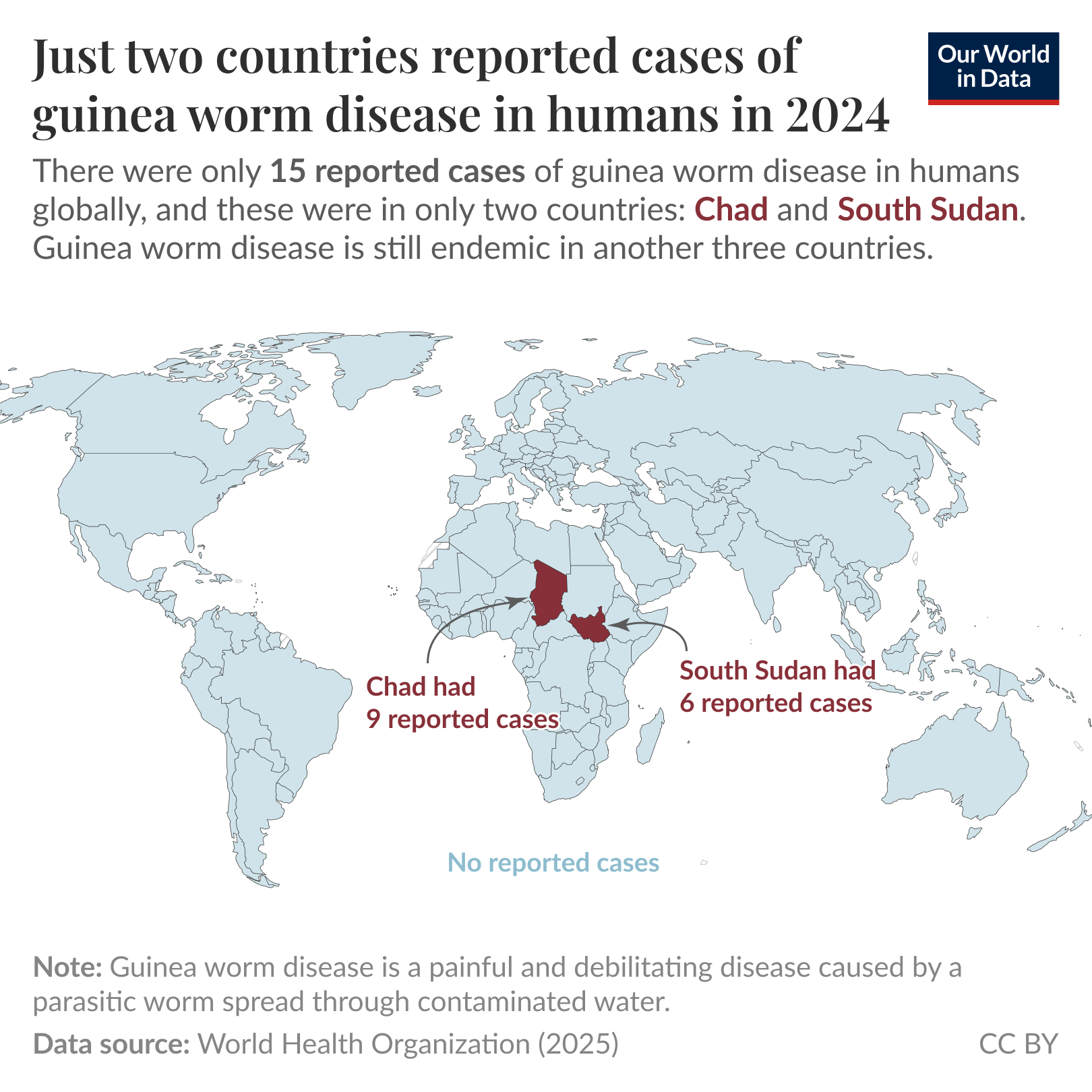
When you look at the countries with confirmed cases in 2025, they tell a story about poverty, conflict, and limited access to clean water. Chad reported four cases. Ethiopia reported four cases. South Sudan reported two cases. That's it. The entire world.
But here's the catch: humans are only part of the problem. Animals are the complicating factor. In 2025, animal cases were detected in six countries: Chad with 147 cases in animals, Mali with 17, Cameroon with 445, Angola with 70, Ethiopia with 1, and South Sudan with 3. This is where eradication becomes genuinely complex.
For decades, Guinea worm was thought to be exclusively a human disease. Then researchers realized that animals could also harbor the worm, particularly domesticated animals like cattle, dogs, and other livestock. These animal reservoirs complicate eradication because you can't just vaccinate dogs or treat them with medications the way you would humans. You have to prevent them from drinking contaminated water too. In pastoralist communities, this means providing alternative water sources for livestock, which requires infrastructure investment in areas that often lack basic health facilities.
Geographic Reduction: From 21 Countries to 6
The geographic contraction of Guinea worm is worth highlighting because it shows the eradication program's success in waves. When the campaign started in 1986, the disease was present in 21 countries across Africa and Asia. By 1995, it had been eliminated from Asia except for a few cases in India. The last endemic area in India was in the Rajasthan region, where the final case was recorded in 1999. That's when the geography of Guinea worm became almost exclusively African, which actually helped focus eradication efforts.
By 2000, only 15 African countries still had cases. By 2010, that number had dropped to 4. For years, it seemed like South Sudan and Chad would never reach zero due to ongoing civil conflicts that disrupted disease surveillance and prevention programs. But even in conflict zones, the eradication program persisted. Health workers continued their case investigations and public education. That's the unglamorous reality of eradication work: it doesn't stop because a country is at war.
The Mathematical Journey: Numbers That Reveal Everything
The Calculation of Prevented Cases
Let's think about what 100 million prevented cases actually means. The eradication program estimates this based on historical infection rates and demographic projections. If you take the initial 3.5 million cases in 1986 and project forward what would have happened without intervention, accounting for population growth in endemic regions, you get staggering numbers.
Consider this formula for estimating prevented cases:
If you assume even a modest 2% annual growth in cases (due to population increase in endemic areas), without intervention you'd expect tens of millions more cases. The fact that cases have declined by over 99.7% is numerically stunning.
The Exponential Decline Pattern
Looking at the data trajectory, Guinea worm cases have followed what epidemiologists call a "log-linear decline." That means if you plot the cases on a logarithmic scale, they form a relatively straight line going downward. This pattern suggests that the eradication program has maintained consistent pressure on transmission despite changing circumstances and challenges.
Year-to-year, the improvements looked like this roughly: from 3.5 million in 1986 to 892,000 by 1989 (initial rapid decline), then to 100,000 by 1994, to 10,000 by 2005, to 1,000 by 2011, to fewer than 100 by 2015, and finally to single digits by the early 2020s. The last mile is always hardest in eradication. Going from 100 cases to 10 cases took longer and required more effort per case than going from 1 million to 100,000.
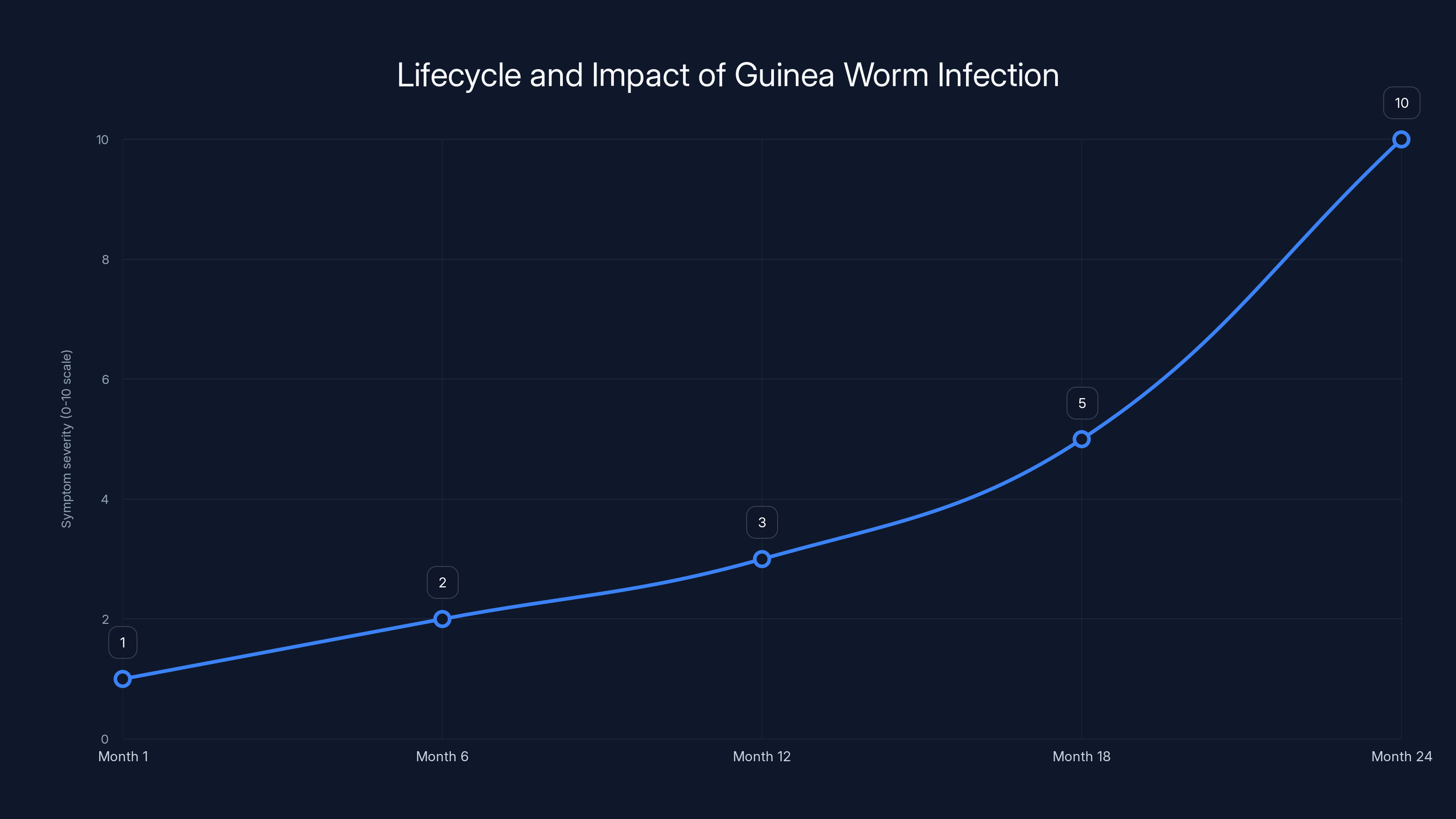
The severity of symptoms increases dramatically in the second year of infection, peaking when the blister forms and ruptures. Estimated data based on typical infection progression.
The Strategy That Worked: A Masterclass in Practical Public Health
Why Didn't They Just Make a Vaccine?
This is the question that surprises most people when they learn about Guinea worm eradication. In the age of vaccines, why didn't we develop a Guinea worm vaccine? The answer reveals something important about public health strategy.
First, there's a biological reality: developing an effective vaccine against parasitic worms is substantially harder than developing vaccines against viruses or bacteria. Parasitic organisms are larger, more complex, and can evade the immune system in sophisticated ways. The parasites that cause sleeping sickness, leishmaniasis, and schistosomiasis have resisted vaccine efforts for decades. A Guinea worm vaccine was theoretically possible but would have taken years to develop and test.
Second, there's an economic reality: Guinea worm disproportionately affects the world's poorest populations. Vaccine development for diseases primarily affecting poor countries has historically gotten less private sector investment. Companies invest where they can recoup costs through sales, and populations in sub-Saharan Africa couldn't generate sufficient revenue.
Third, there's a practical reality: you don't need a vaccine if you can break transmission chains another way. And for Guinea worm, breaking transmission turned out to be simpler than inventing a vaccine.
Water Interventions: The Simple Solution That Works
The core of the Guinea worm eradication strategy is laughably simple: clean water access. The parasite can only survive in water with specific temperature ranges and with copepods present. It cannot survive in boiled water. It cannot survive in filtered water if the filter is fine enough to catch copepods.
The eradication program distributed cloth filters (called "sieve cloths" or "water filters") to communities. These filters, made of tightly woven nylon mesh, are small enough to prevent copepods from passing through. A woman in an endemic village uses the filter every time she draws water. It's not a one-time solution but an ongoing practice. The cloth costs pennies to manufacture. It's simple enough for anyone to use. It doesn't require electricity, literacy, or trust in complex medical technology.
Parallel to filtration, the program promoted boiling water for drinking and cooking. Again, simple. Effective. But behavior change is hard. Even when people know boiling prevents Guinea worm, they don't always do it consistently because fuel is expensive, time is scarce, and other concerns seem more pressing.
Then came the third element: water source improvement. Rather than asking people to consistently filter or boil water, why not provide clean water sources that don't contain copepods? This meant building or improving water wells, boreholes, and protected springs. These interventions required more capital investment but had the benefit of preventing multiple water-borne diseases, not just Guinea worm.
The Cash Incentive System: Brilliant In Its Simplicity
Here's where the program became almost game-theoretic. The Carter Center offered cash rewards for reporting suspected Guinea worm cases. In communities where infection rates are dropping, this creates an incentive structure that cuts through communication barriers and encourages vigilance.
Think about how this works: you live in a village where Guinea worm is rare but not extinct. You know someone with a suspicious blister. Do you report it? That might bring scrutiny. That might mean your friend gets investigated. In some contexts, it might even seem like snitching. But if reporting comes with a cash reward, and if that cash represents meaningful income in a subsistence economy, reporting becomes individually rational.
These reports generate case investigations. Eradication workers travel to the reported case, confirm the diagnosis (which is straightforward: you can usually see the worm emerging from the skin), and then investigate the water source. They identify which water source caused the infection, implement immediate containment measures (treating the water, educating the community not to use it), and prevent secondary transmission.
Every case becomes a data point and a vector for surveillance. This approach has parallels to modern disease surveillance systems but predates digital technology. It's old-fashioned detective work scaled across entire regions.
The Carter Center: The Organization That Wouldn't Quit
From Presidential Effort to Global Mission
President Jimmy Carter launched the eradication initiative in 1986, long before it became fashionable for former presidents to lead global health campaigns. The Carter Center didn't have the budget of the World Health Organization or the Gates Foundation. It had commitment and credibility.
What made the Carter Center effective wasn't resources alone but persistence. When progress stalled, they didn't pivot to a different disease. When funding was uncertain, they maintained operations. When new obstacles emerged (like animal transmission), they adapted rather than declared defeat.
The organization's geographic presence was crucial. They didn't run Guinea worm eradication from Washington, D.C. or Geneva. They embedded staff in endemic countries. They built relationships with village health workers, community leaders, and families affected by the disease. This presence ensured continuity even when political situations changed or conflicts disrupted normal operations.
The Role of Local Health Workers
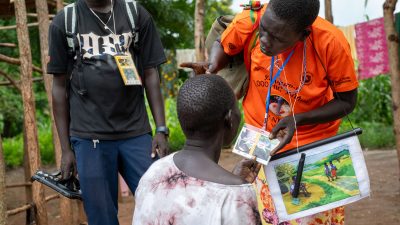
Eradication didn't happen because international experts parachuted in and fixed things. It happened because village health workers, many with minimal formal education, became the frontline of eradication. These workers received training on case identification, community education, and water source management. They became trusted advisors in their communities in ways that foreign experts could never be.
The program invested heavily in training and supervision of these workers. Regular meetings ensured that case reporting standards remained consistent. Feedback loops meant that if eradication strategies weren't working in one area, they could be adjusted. This bottom-up approach meant that the campaign adapted to local contexts rather than imposing a one-size-fits-all solution.
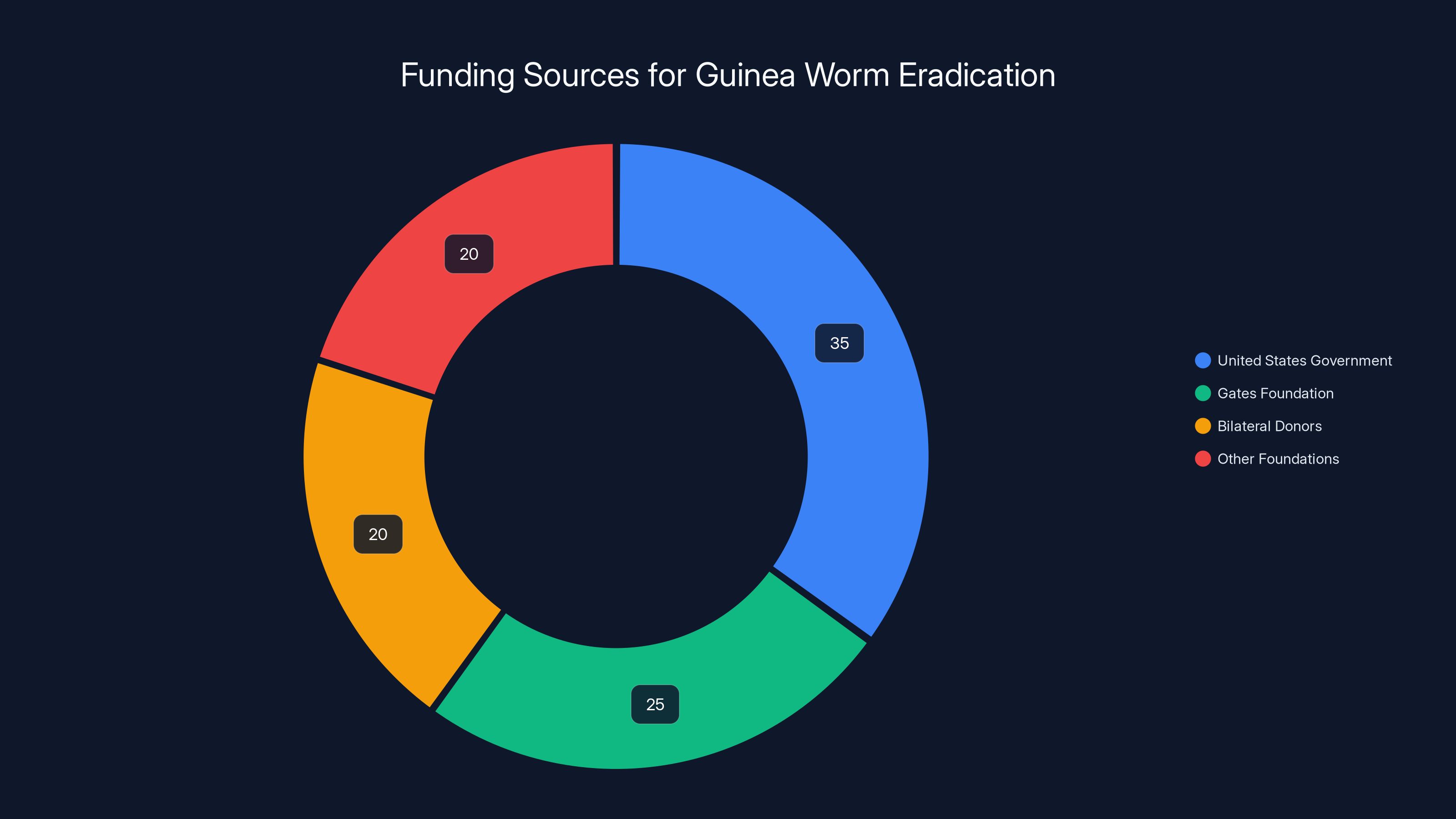
Estimated data shows diverse funding sources for Guinea worm eradication, with the US government and Gates Foundation as major contributors. This diversity provided stability to the program.
The Remaining Cases: Why Zero Remains Elusive
The South Sudan Factor: Conflict as a Disease Vector
South Sudan, with just two human cases in 2025, represents the paradox of modern eradication. The country has experienced civil conflict on and off since independence. Conflict disrupts surveillance, displaces populations, and makes healthcare workers' jobs infinitely more difficult. Yet even amid conflict, Guinea worm cases have declined.
However, the last cases are often in conflict zones because those areas have the weakest health surveillance systems. Health workers can't always access all communities. Population movements make contact tracing difficult. Water sources might be contaminated by displaced populations or broken infrastructure.
Eradicating Guinea worm in South Sudan requires not just disease control measures but also security. It requires negotiating access with parties to the conflict. It requires maintaining case reporting systems when normal governance is compromised. It's a reminder that disease eradication is inseparable from broader development and security contexts.
Chad's Persistent Problem
Chad, with four human cases and 147 animal cases in 2025, shows another challenge: the Sahel region's environmental and economic constraints. Chad is semi-arid, with significant water access challenges unrelated to Guinea worm. Communities depend on seasonal water sources. During dry seasons, people and animals cluster around available water points, increasing transmission risk.
The eradication program in Chad has focused heavily on installing water infrastructure during dry seasons. But infrastructure in a poor, conflict-affected country is expensive to build and maintain. A broken borehole might take months to repair if spare parts aren't available locally. This means that even areas that had achieved zero cases can experience resurgence if water infrastructure deteriorates.
Animal Reservoirs: The Complication That Makes Perfect Eradication Harder
Cameroon's 445 animal cases in 2025 highlight the animal transmission problem. When the eradication program was purely focused on humans, mathematical models suggested zero was achievable through behavioral change and water access improvements. But the discovery of animal reservoirs complicated the endgame.
Why do animals get infected? The same reason humans do: drinking contaminated water. In pastoralist regions, livestock and humans often share water sources. A cattle herd can become infected and then serve as a transmission reservoir even after human cases are eliminated. If a herder's animal drinks from an infected water source, larvae develop in the animal's body. If someone then drinks water contaminated by that animal, human infection can recur.
Eradicating animal infections requires preventing animals from accessing contaminated water. This means providing alternative water sources for livestock, which requires even more infrastructure investment. It means understanding animal behavior and pastoral practices. It means working with herders and livestock owners who may not initially see Guinea worm prevention as their priority.

Public Education: Changing Behavior at Scale
Teaching People About a Disease They've Never Heard Of
Most people in Guinea worm endemic areas had never heard of the disease when the eradication program began. They knew it as "something old women got" or explained it through cultural or spiritual frameworks that had nothing to do with parasitic infections. Public education couldn't simply distribute information; it had to change how people understood their own illness.
The program used multiple channels: community meetings, radio broadcasts (where available), drama groups that performed in villages, and most importantly, community health workers who lived in endemic areas and could have repeated conversations with people.
Education focused on several key messages: Guinea worm is caused by drinking contaminated water; you can prevent it by filtering or boiling water; if someone has a suspicious blister, that person shouldn't put their leg in water; reporting cases helps prevent disease. None of this is complex intellectually, but communicating it effectively across diverse communities, in multiple languages, with different cultural contexts, required sustained effort.
Wound Care Practices: The Unsexy But Essential Intervention
If someone already has Guinea worm, the priority shifts from prevention to management. Traditional wound care often involved keeping the blister moist and popping it, which seems logical given the pain but accelerated parasite transmission. The eradication program taught people to keep wounds clean and dry, to cover them, and to avoid putting them in water.
Providing clean cloths for wound wrapping might seem trivial, but in communities with limited supplies, it made a difference. Teaching family members how to care for infected relatives without transmitting the parasite to others was crucial for breaking transmission chains.

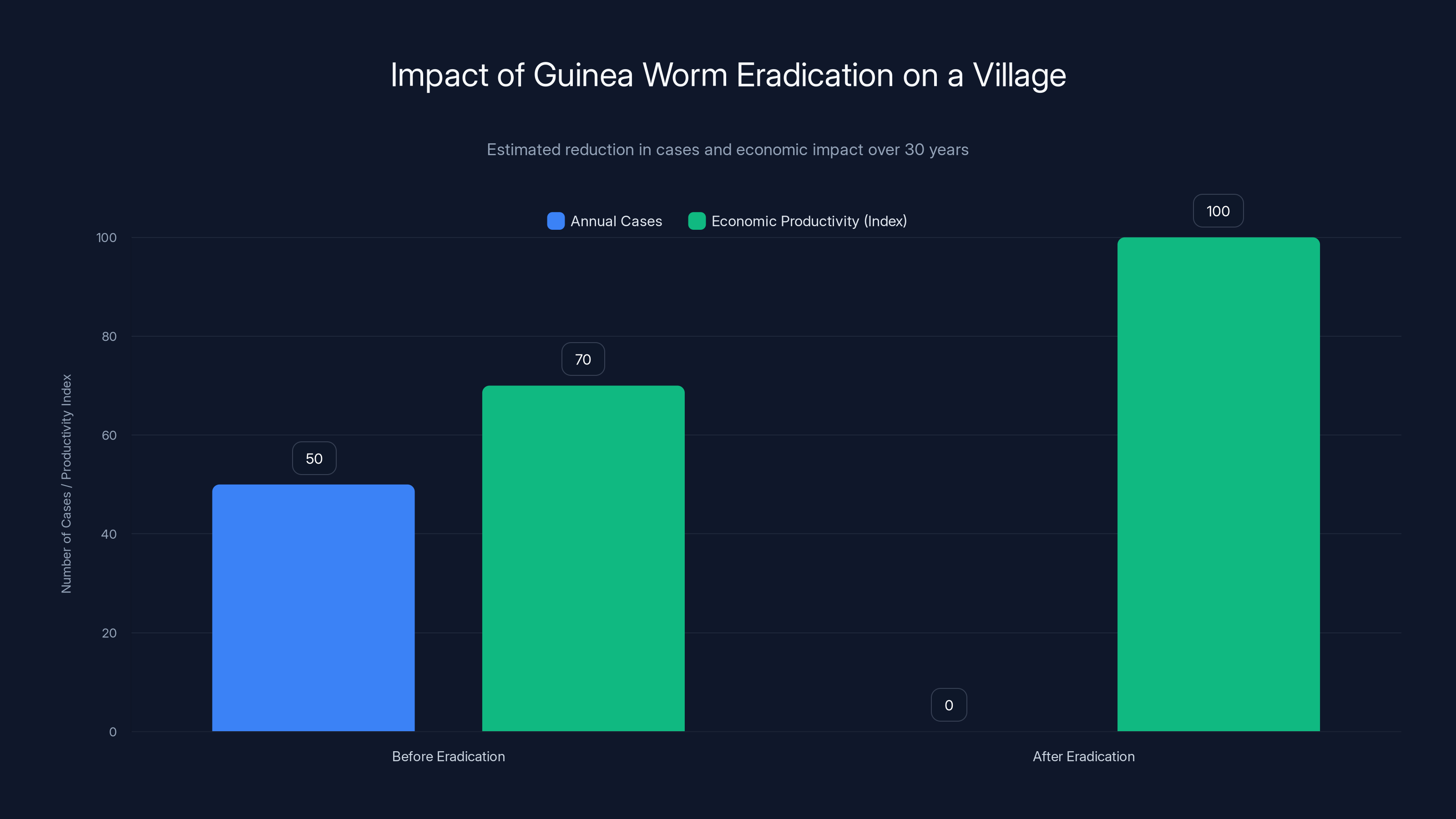
Estimated data shows that eradication of Guinea worm in a village prevents 50 cases annually, significantly boosting economic productivity. The productivity index improves from 70 to 100, indicating enhanced community functioning.
The International Response: Coordination Across Borders
The World Health Organization's Supporting Role
While the Carter Center led the eradication effort, the World Health Organization provided crucial support through certification of Guinea worm elimination. Once a country hadn't reported cases for a year, an independent verification team would visit and confirm that transmission had been interrupted. This certification mattered because it allowed countries to stop surveillance efforts confidently.
The WHO also coordinated with national health ministries, helping countries integrate Guinea worm surveillance into broader disease monitoring systems. As cases declined, surveillance shifted from dedicated Guinea worm programs to integrated reporting through existing health infrastructure.
Bilateral and Multilateral Funding
Donor governments and foundations supported the eradication program financially. The United States government provided significant funding. The Gates Foundation supported specific initiatives. Bilateral donors focused on particular regions. This combination of funding sources meant the program wasn't dependent on any single funder, which provided stability.
However, funding for disease eradication in final phases is often difficult to secure. Donors like funding new initiatives with visible impact. Funding the last 10% of an eradication looks less impressive than funding a campaign that reduces cases by 90%, even though eliminating the final cases requires equal or greater effort.
Cross-Border Challenges
Guinea worm doesn't recognize national boundaries. Rivers and water sources flow across borders. Pastoral populations migrate seasonally, crossing international boundaries with their livestock. Effective eradication required coordination between countries, which meant regular regional meetings, shared data, and mutual support.
When South Sudan split from Sudan in 2011, the eradication program adapted its regional coordination. When new conflicts emerged, eradication staff found ways to maintain surveillance. This adaptability was possible because the program had built institutional relationships and trained numerous local partners who could continue work even when external circumstances changed.

The Biological and Epidemiological Realities
Understanding Transmission: The Copepod Dependency
Guinea worm transmission has a critical biological bottleneck: the parasite can only complete its lifecycle in freshwater copepods. This isn't a flexible parasite that can evolve new transmission routes. It's locked into this specific pathway.
This dependency is eradication's greatest asset. As long as water is copepod-free, the parasite cannot persist. You can't have latent Guinea worm cases. You can't have asymptomatic carriers. Once the worm emerges, it either transmits to others through water contact or it dies. There's no hidden reservoir of infection.
Some parasitic diseases are difficult to eradicate precisely because they can hide. Malaria parasites can lie dormant in the liver. Schistosomiasis parasites can survive in snails for months. Guinea worm has no such capacity for persistence in the absence of water transmission.
Why Eradication Is Possible at All
Most parasitic diseases haven't been eradicated because they have either animal reservoirs (like sleeping sickness, which infects livestock), environmental stages that are difficult to eliminate (like schistosomiasis, where snails harbor parasites), or extreme adaptability (like malaria, where the parasite evolves drug resistance).
Guinea worm is eradicable because it has relatively few reservoirs (mainly humans, now known to include some animals), its transmission route is straightforward, and it has no capacity to evolve resistance to clean water. This doesn't mean eradication is easy, only that it's technically feasible.

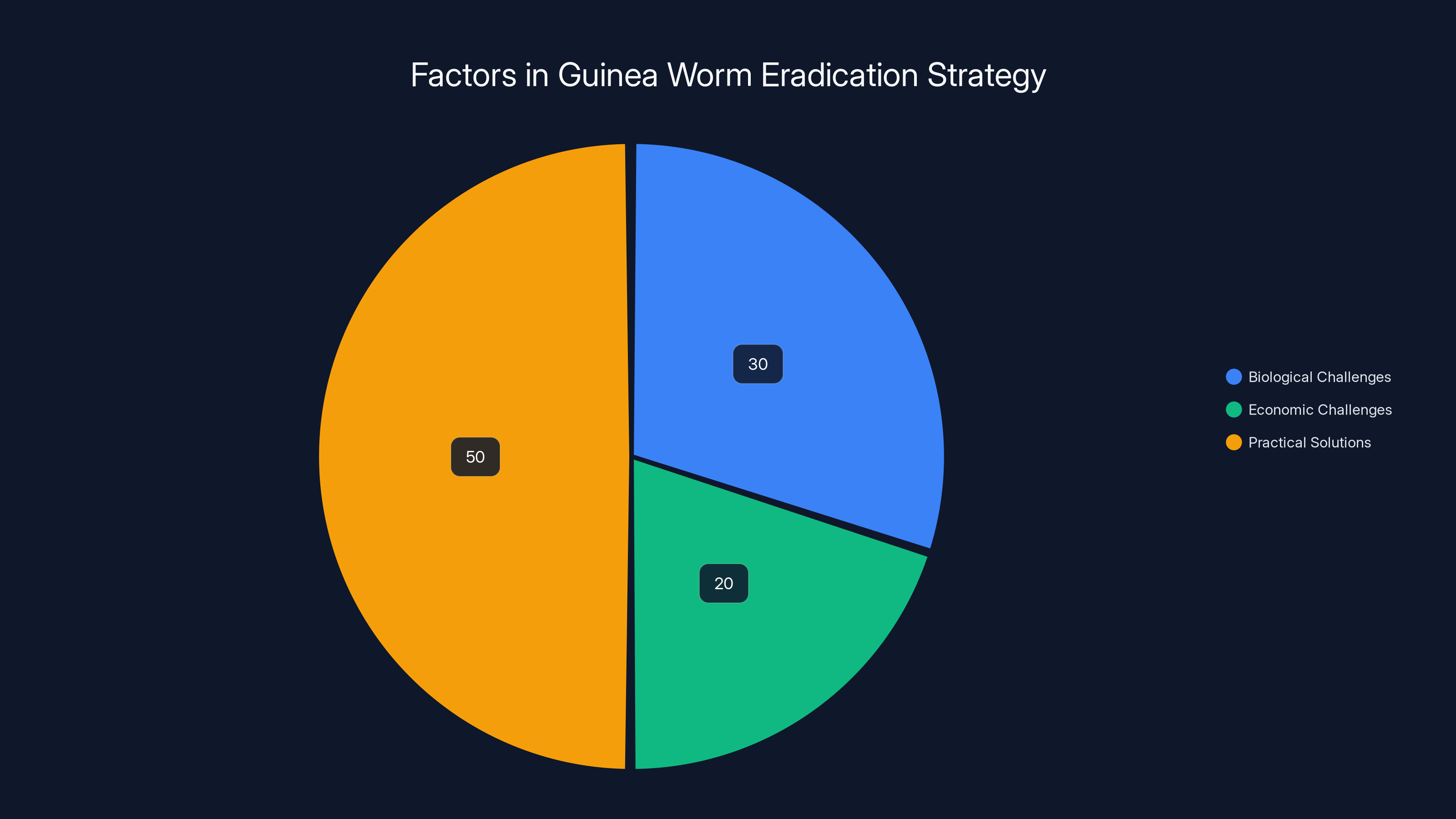
The Guinea worm eradication strategy focused 50% on practical solutions like clean water access, with lesser emphasis on biological and economic challenges. Estimated data.
The Animal Question: Why Dogs and Cattle Complicate Eradication
How Animals Get Infected
The discovery that animals could get Guinea worm came as a surprise to the eradication community. The first animal case was documented in a dog in northern Ghana in the 1990s. The dog had likely drunk water contaminated with copepods containing Guinea worm larvae. The parasite developed in the dog the same way it develops in humans, eventually causing a painful emergence of a worm from the skin.
Once animal reservoirs were documented, the mathematical picture of eradication changed. Even if you reached zero human cases, animals could maintain transmission. Someone could drink water contaminated by an infected animal. The cycle could restart.
Most animal infections documented have been in domestic dogs and occasionally cattle. This is somewhat fortunate because these are animals that humans have some ability to influence. You can provide alternative water sources for livestock. You can treat infected animals (though it's not easy). You can prevent dogs from accessing contaminated water sources.
The Pastoralist Problem
In regions with pastoral communities, eradicating Guinea worm from animals is substantially harder than eradicating it from humans. Pastoralists depend on livestock for survival. They can't always control where animals drink. During seasonal migrations, herds might access water sources that the eradication program hasn't identified as contaminated.
The Sahel region, parts of East Africa, and areas of Central Africa present particular challenges. In these regions, livestock are essential economic assets, water is inherently scarce, and infrastructure is limited. Eradication programs have to work within pastoral livelihood systems, not against them.
Successful animal Guinea worm control in some regions has required providing livestock with alternative water sources during high-risk periods, treating infected animals when they're identified, and educating herders about the risk. But scaling these interventions across multiple countries and competing pastoral priorities remains difficult.
Lessons from Guinea Worm for Other Eradication Efforts
What Polio Can Learn
Polio eradication has stalled with just a handful of cases in Afghanistan and Pakistan. The strategies are similar to Guinea worm: case detection and vaccination, public education, surveillance, and targeted interventions in remaining endemic areas. But polio has been eradicated in most of the world for decades, and the final cases have proven remarkably resistant to elimination.
The Guinea worm experience suggests that persistence matters more than initial resources. The Carter Center has maintained the Guinea worm program through decades of competition with other priorities. No moment of dramatic breakthrough arrived; progress has been incremental and steady. Polio eradication might benefit from the same long-term commitment approach, though there are structural differences (polio can be stopped through vaccination in years, while Guinea worm required sustained surveillance and behavioral change).
What Sleeping Sickness Could Attempt
African trypanosomiasis (sleeping sickness) infects perhaps a few thousand people annually, far fewer than Guinea worm at its worst. But sleeping sickness has proven harder to eradicate because it infects animals (which serve as reservoirs), exists in remote forest areas with limited healthcare, and requires treating cases with complex drugs. Guinea worm's lesson here is that eradicating diseases with animal reservoirs requires addressing the animal side systematically, not as an afterthought.
The Infrastructure Principle
Guinea worm eradication succeeds through infrastructure: water wells, surveillance systems, distribution networks for filters and medicines. The disease didn't disappear because of a single breakthrough but because sustained investment created systems that maintained transmission interruption.
This principle applies to other diseases. Malaria control requires insecticide-treated bed net distribution systems. Tuberculosis control requires diagnostic and treatment infrastructure. These systems are boring compared to vaccine breakthroughs, but they're essential for eradication. The Guinea worm story is partly a story about boring infrastructure done right at scale.

The 2025 Milestones and What They Mean
Crossing Below 10 Cases: A Psychological Threshold
The achievement of just 10 cases in 2025 crosses a psychological threshold. Single-digit cases mean that eradication has moved from "likely" to "nearly certain." It means that every remaining case can be individually tracked and managed. It means success has transitioned from a probability to a timeline question.
In eradication efforts, crossing below 10 cases typically signals that the program is in the "endgame." Remaining cases are often in particularly difficult contexts: conflict zones, areas with weak surveillance, communities resistant to behavior change. But with only 10 cases, the program can potentially allocate resources per case rather than per region.
Zero Is Not The Same As Eradication
Reaching zero cases is a milestone, but true eradication requires maintaining zero for a period (typically at least 3-4 years) with continued surveillance to ensure no resurgence. Smallpox required certification of zero cases globally with continued monitoring before the world health community declared eradication complete.
Guinea worm will likely follow a similar path. Once zero human cases are confirmed, surveillance will likely continue at lower intensity for several years. Health systems will monitor for any suspicious cases that might represent re-emergence. The infrastructure for detection will remain in place until absolute confidence in eradication is achieved.
Timeline to Complete Eradication
If the provisional 10 cases in 2025 holds through confirmation, and if similar progress continues, zero human cases could be achieved as early as 2026 or 2027. But reaching zero doesn't mean eradication is complete. Health officials will likely wait 3-4 additional years of zero cases before declaring official eradication.
This means the complete eradication of Guinea worm could be officially certified by approximately 2030, potentially earlier if no cases recur. That would mean 44 years from the program's start to formal eradication. It's a long timeline by the standards of modern medicine, but it's faster than it took to eradicate smallpox, which required continuous vaccination campaigns for nearly two centuries before the final case was documented in 1977.
The Surveillance Question: How Do You Know You've Really Won?
Post-Eradication Surveillance Requirements
Once a disease is officially eradicated, surveillance doesn't completely stop. Health systems need to remain alert for any potential resurgence. For Guinea worm, this means continuing to train health workers to recognize suspicious blister cases, maintaining reporting systems, and periodic verification of zero cases in previously endemic areas.
The cost of post-eradication surveillance is much lower than active eradication programs, but it's not free. Countries have to decide to maintain this vigilance even after the disease has disappeared. Some countries have reduced surveillance too quickly after achieving elimination, only to have diseases resurge. Maintaining surveillance discipline in the absence of visible disease is psychologically and institutionally challenging.
The Laboratory Capacity Question
With very few cases remaining, laboratory confirmation of suspected cases has become increasingly important. A suspected case needs confirmation before resources are mobilized for response. This requires maintaining laboratory capacity and expertise in regions where cases are rare.
Laboratory confirmation of Guinea worm involves identifying the worm in blister fluid or from the emerging worm itself. It's not as sophisticated as some diagnostics, but it requires trained personnel and functional laboratory facilities. As cases drop to near-zero, maintaining this capacity becomes a significant portion of surveillance costs.
Global Health Cooperation: Who's Involved in Final Stages
The Partnership Structure
The Guinea worm eradication program involves the Carter Center, the World Health Organization, national health ministries in endemic countries, and numerous international partners. This multi-stakeholder approach has been crucial for maintaining momentum and credibility.
Particular countries have become particularly important in final stages. Ethiopia's public health system has been crucial for investigating and managing cases in that region. Chad's commitment, despite limited resources, has kept eradication on track. South Sudan, even amid conflict, has maintained enough surveillance to identify and prevent transmission.
Regional Coordination Mechanisms
Eradication programs have established regional coordination meetings where countries share data, discuss challenges, and align strategies. These regional mechanisms have become increasingly important as cases decline because remaining cases require cross-border coordination. An individual case in one country might represent exposure from another country's water sources.
The Role of Academic and Research Institutions
Universities and research institutes have contributed to eradication by studying the biology of remaining cases, analyzing transmission patterns, and suggesting targeted interventions. Research has revealed the animal transmission pathway, helped understand why certain areas remain endemic, and provided evidence for prioritizing interventions.
The Human Cost and Prevented Suffering
What 100 Million Prevented Cases Actually Means
The eradication program's estimate of 100 million prevented cases is staggering, but it's abstract. What does that actually mean in human terms?
Each prevented case represents someone who didn't experience months of agonizing pain. It represents a child who could still work in fields or attend school rather than being incapacitated. It represents a family that didn't lose income during a sick family member's long recovery. It represents a community that could function normally during Guinea worm seasons rather than having significant portions of the population incapacitated.
Take a village of 1,000 people where Guinea worm attacked 5% annually before eradication. That's 50 cases per year. Now imagine that over 30 years before eradication would have occurred naturally. That's 1,500 cases in one village alone, each meaning an individual person experiencing severe pain for months. Now multiply that across hundreds of thousands of villages across 21 countries.
The prevented suffering is quantifiable in terms of cases but profound in terms of human dignity and economic development. Communities that were annually crippled by Guinea worm season are now productive year-round.
Economic Benefits Beyond the Numbers
Guinea worm's eradication has contributed to development in affected regions, though quantifying this is difficult. Children who attend school rather than being incapacitated by Guinea worm are more likely to become productive adults. Communities with stable populations are more likely to invest in long-term development. This is particularly true in the poorest regions, where losing 5% of the population annually to incapacity dramatically impacts economic growth.
The Psychological Impact of Eradication Success
For communities that lived with Guinea worm for generations, eradication is transformative in ways that go beyond disease prevention. It's evidence that health improvement is possible, that behavior change works, and that international cooperation can achieve remarkable things. This psychological shift can generate momentum for tackling other health problems.

Challenges in the Final Sprint
Funding Fatigue in the Endgame
Paradoxically, eradication efforts often face their worst funding challenges at the end. Early in a campaign, funding flows because progress is visible and dramatic (going from 3 million to 1 million cases is visible success). Near eradication, funding is harder because a program preventing 10 cases per year looks less impressive than one preventing millions.
Yet the final cases often require as much funding and effort as the millions of cases at the beginning. Chad's 147 animal cases require veterinary surveillance, livestock water infrastructure, and sustained education. Without adequate funding, progress stalls.
Maintaining Focus on Forgotten Diseases
Guinea worm has never captured public imagination the way polio or smallpox do. Media coverage is sparse. Politicians in wealthy countries don't face domestic pressure about Guinea worm eradication. This means maintaining political will and funding commitment requires exceptional leadership and consistent advocacy.
The Carter Center's role in maintaining focus on Guinea worm cannot be overstated. Without the organization's leadership, Guinea worm eradication could have stalled decades ago.
Surveillance Gaps in Conflict Regions
The remaining 10 cases are almost certainly concentrated in conflict-affected regions or particularly remote areas. Maintaining surveillance in South Sudan or northern Chad is difficult. Health workers might not be able to safely access some communities. Population movements make contact tracing unreliable. These operational challenges make eradicating the final cases genuinely difficult despite their small number.
Behavioral Resistance and Traditions
In some communities, traditional water sources or bathing practices persist despite education about transmission. Religious or cultural practices might conflict with prevention measures. Some communities trust traditional healers more than government health workers. These barriers require patient, sustained engagement rather than top-down mandates.
Looking Forward: From Eradication to Certification
The Path to Official Eradication Declaration
Once confirmed zero cases are achieved, the international health community will likely establish an independent verification commission to certify eradication. This commission will review surveillance data, visit endemic areas, and verify that transmission has been interrupted sustainably. Only after this verification would Guinea worm be officially declared eradicated.
This process took several years for smallpox. For Guinea worm, given the complexity of animal reservoirs, certification might require 3-4 years of confirmed zero cases with maintained surveillance.
Post-Eradication Opportunities
Once Guinea worm is eradicated, the infrastructure, expertise, and partnerships developed for eradication can pivot to other diseases. The surveillance systems, health worker networks, and community relationships established for Guinea worm could support control of other parasitic diseases. The Carter Center might focus its disease eradication efforts on other targets, though Guinea worm eradication will likely remain its legacy achievement.

FAQ
What is Guinea worm disease?
Guinea worm disease (dracunculiasis) is a parasitic infection caused by the roundworm Dracunculus medinensis. The disease is acquired by drinking water contaminated with copepods (small crustaceans) harboring the worm's larvae. Over approximately one year, an adult worm grows inside the body and eventually emerges through a painful blister, typically on the legs or feet. The disease causes severe pain and can lead to complications including secondary bacterial infections, sepsis, and permanent disability. Importantly, there is no vaccine or medication that kills the worm; treatment is purely supportive while waiting for the worm to naturally emerge.
How is Guinea worm transmitted?
Guinea worm transmission begins when a person drinks water contaminated with copepods carrying Guinea worm larvae. Once swallowed, the larvae burrow through the intestinal wall and migrate through body tissues for several weeks or months. The adult worm eventually reaches the skin's surface and creates a painful blister, usually on the lower extremities. When an infected person puts their blister in water to ease pain (which is almost inevitable given the severity), the worm releases hundreds of thousands of larvae into the water. If that water isn't treated and is consumed by others, transmission continues. The parasite cannot be transmitted directly from person to person or through food; water is the essential transmission vehicle.
What are the main symptoms of Guinea worm?
The symptoms of Guinea worm disease develop gradually over the course of a year. Early symptoms, occurring in the first weeks after infection, can include mild abdominal pain, diarrhea, or nausea as the larvae migrate through the intestines. These symptoms are often so mild that people don't realize they're infected. The most dramatic symptom is the emergence of the adult worm through a painful blister, typically occurring 12 to 14 months after infection. The blister causes severe localized pain, and the worm emergence process can take 2 to 3 months. Secondary complications can include bacterial infections of the blister, sepsis, tetanus (if the wound isn't kept clean), and joint contractures if the worm emerges near joints.
Why is Guinea worm eradication significant?
Guinea worm eradication is significant for multiple reasons. First, if successfully completed, it would be only the second human disease to be eradicated, after smallpox in 1980. This achievement would demonstrate that with sustained commitment, even diseases affecting the world's poorest populations can be eliminated. Second, the eradication campaign has prevented an estimated 100 million cases since 1986, representing immense reduction in human suffering. Third, the strategy used for Guinea worm eradication—focusing on water access, community engagement, and behavioral change rather than waiting for pharmaceutical solutions—provides a model for controlling other neglected tropical diseases. Fourth, the success demonstrates that global health cooperation works when sustained for decades, contradicting narratives that international health efforts inevitably fail.
What interventions were most effective for reducing Guinea worm?
Multiple interventions contributed to the dramatic reduction in Guinea worm cases. Water source improvement, including construction of boreholes and protected wells that don't contain copepods, eliminated transmission in regions where implemented. Distribution of cloth filters (sieve cloths) that prevent copepods from passing through enabled households to filter their own water safely. Public education about boiling water, filtering water, and preventing infected individuals from contaminating water sources changed community behavior. Cash reward systems for reporting cases incentivized surveillance and case identification. Training of village health workers enabled detection and response to cases at the community level rather than waiting for people to reach formal health facilities. These interventions worked synergistically: water improvements prevented most transmission, filters and boiling provided backup prevention, and surveillance ensured rapid response to any remaining cases. The eradication program emphasized matching interventions to local contexts rather than applying a single strategy universally.
How many cases of Guinea worm remain today?
As of 2025, provisional data indicates just 10 human cases of Guinea worm globally, a historic low. These cases were identified in three countries: four in Chad, four in Ethiopia, and two in South Sudan. However, animal cases remain more common, with 445 cases detected in animals in Cameroon, 147 in Chad, 70 in Angola, 17 in Mali, 3 in South Sudan, and 1 in Ethiopia in 2025. The discovery that animals can harbor Guinea worm complicated eradication because animal reservoirs could theoretically perpetuate transmission even after human cases reach zero. Nevertheless, the dramatic decline from 3.5 million cases in 1986 represents one of public health's greatest achievements, and complete eradication appears probable within the next few years if current progress continues.
What challenges remain for complete eradication?
Despite dramatic progress, several challenges complicate final eradication. First, remaining human cases are concentrated in conflict-affected regions like South Sudan and Chad, where health surveillance is difficult and health worker security cannot be guaranteed. Second, animal reservoirs of Guinea worm require preventing livestock and dogs from accessing contaminated water, which demands veterinary surveillance and pastoral community engagement in regions where water access is already limited. Third, funding for eradication programs becomes harder to secure in the endgame phase when annual case numbers are small, even though final cases require equal resources. Fourth, behavioral changes must be maintained indefinitely in some communities to prevent resurgence. Fifth, population movements due to conflict or pastoralist migration can potentially reintroduce the parasite to areas that had been free of transmission. Addressing these challenges requires sustained commitment, adequate funding, continued surveillance capacity building, and maintained international cooperation.
Is there a vaccine for Guinea worm?
No vaccine for Guinea worm currently exists. The disease has been eradicated not through vaccination but through prevention of transmission via water interventions and behavior change. Early in the eradication program, researchers considered developing a vaccine, but parasitic diseases are difficult vaccine targets because parasites are larger and more complex than viruses or bacteria and have sophisticated immune evasion mechanisms. Vaccine development for diseases primarily affecting poor populations also faces challenges because profit incentives for commercial development are low. Importantly, eradication was achieved without a vaccine by making water transmission impossible through filtration, boiling, water source improvements, and larval treatment. This demonstrates that eradication doesn't require pharmaceutical solutions and underscores that many health problems can be solved through infrastructure, behavior change, and public health commitment.
What happens after Guinea worm is eradicated?
Once Guinea worm eradication is confirmed, the international health community will likely establish an independent verification commission to certify eradication, similar to the process used for smallpox. This verification will require confirmation of zero cases across all regions with maintained surveillance for typically 3-4 years. After official certification, full surveillance can scale back but won't completely stop; health systems will remain alert for any potential resurgence. The infrastructure, expertise, and partnerships developed for Guinea worm eradication can then pivot to controlling other parasitic diseases, such as schistosomiasis or lymphatic filariasis. The Carter Center, which has been central to Guinea worm eradication, will likely transition to pursuing eradication or elimination of other diseases. Guinea worm eradication will remain a significant achievement in public health history, demonstrating that sustained commitment over decades can achieve remarkable outcomes.

Conclusion: A Forgotten Victory That Matters
Guinea worm eradication is the public health story nobody knows but everyone should. It's a story about decades of unglamorous work: village health workers visiting remote communities, people learning to filter water, cash incentives motivating surveillance, bureaucrats coordinating across conflict zones. It's a story about staying committed when funding is uncertain and progress is measured in single-digit case reductions.
When the eradication campaign began in 1986, 3.5 million people suffered from a disease that causes pain so severe that infected individuals cannot work, cannot care for children, cannot participate in their communities. Forty years later, only 10 cases remain. That's not just disease control; that's transformation.
The final cases in Chad, Ethiopia, and South Sudan represent the hardest part of eradication. But the fact that eradication has come this far, despite wars, despite poverty, despite the inherent difficulty of reaching people in remote regions, suggests that the finish line is genuinely visible. Within the next few years, likely before 2030, humanity will have eradicated a second disease. Only smallpox will have been eradicated before it.
That achievement belongs to thousands of health workers in endemic countries, to the Carter Center's sustained leadership, to international organizations that provided support and coordination, and to the millions of people in affected communities who changed their water practices and reported cases. It belongs to community health workers who spent decades visiting villages to prevent a disease that nobody in wealthy countries had ever heard of.
As global health faces new crises and new diseases demand attention, Guinea worm eradication reminds us that persistence works. Innovation matters, but so does infrastructure. Celebrity causes matter, but so do neglected diseases affecting the world's poorest people. Eradication is possible not just through revolutionary breakthroughs but through decades of steady, determined effort to do simple things extremely well.
Zero is the only acceptable number, Adam Weiss of the Carter Center said. That principle, held constant for forty years, is about to produce one of humanity's greatest public health victories. When the final case is confirmed and the paperwork for official eradication is completed, that victory should be celebrated as what it is: proof that the world can still achieve remarkable things when we commit to finishing the job.
Key Takeaways
- Guinea worm cases dropped from 3.5 million in 1986 to just 10 in 2025, representing a 99.7% reduction over 40 years
- Water interventions (filtration, boiling, well construction) rather than vaccines drove eradication success by breaking transmission chains
- Only three countries reported human cases in 2025 (Chad, Ethiopia, South Sudan), while animal reservoirs in six countries complicate final elimination
- The eradication program has prevented an estimated 100 million cases, demonstrating the value of sustained public health commitment
- Guinea worm would be only the second human disease eradicated after smallpox, with complete certification expected around 2030 if progress continues

