![Polio Vaccine Controversy: Why RFK Jr.'s Advisor's Comments Alarmed Doctors [2025]](https://tryrunable.com/blog/polio-vaccine-controversy-why-rfk-jr-s-advisor-s-comments-al/image-1-1769465284188.jpg)
Understanding the Polio Vaccine Controversy That's Dividing Public Health
When Kirk Milhoan, a pediatric cardiologist with minimal vaccine expertise, was named chair of the Advisory Committee on Immunization Practices in December 2025, few outside the medical establishment paid attention. But then he opened his mouth on a podcast, and suddenly, the American Medical Association felt compelled to issue a public statement. What he said wasn't just controversial—it fundamentally threatened decades of disease eradication efforts.
This isn't your typical political disagreement. This is about whether diseases that once paralyzed thousands of Americans should be allowed to return. And the scary part? The person asking the question now has significant influence over federal vaccine policy.
Here's what happened, why it matters, and what it means for public health in America.
The Podcast That Broke Medical Silence
In an interview on "Why Should I Trust You?" Milhoan revealed a worldview that contradicts everything modern medicine understands about vaccine safety and disease prevention. Early in the conversation, he declared: "I don't like established science." Science, he claimed, is "what I observe."
This isn't a minor philosophical difference. Evidence-based medicine is built on systematic observation, peer review, and transparent methodology. What Milhoan was describing is personal observation without the rigorous controls that prevent individual bias from masquerading as truth.
When the podcast hosts pressed him on his stance, Milhoan began making false claims. He linked vaccines to allergies, asthma, and eczema despite the absence of credible evidence. He repeated an unfounded claim that COVID-19 vaccines killed children. Most troublingly, he equated the tiny risk of vaccine side effects with the massive risk of the diseases themselves.
Let's be clear about what this means mathematically. The risk of serious complications from polio (paralysis, death, lifelong disability) is measured in the thousands or tens of thousands of infected people. The risk of a serious vaccine side effect is measured in millions of vaccinated people. They're not even remotely in the same ballpark.
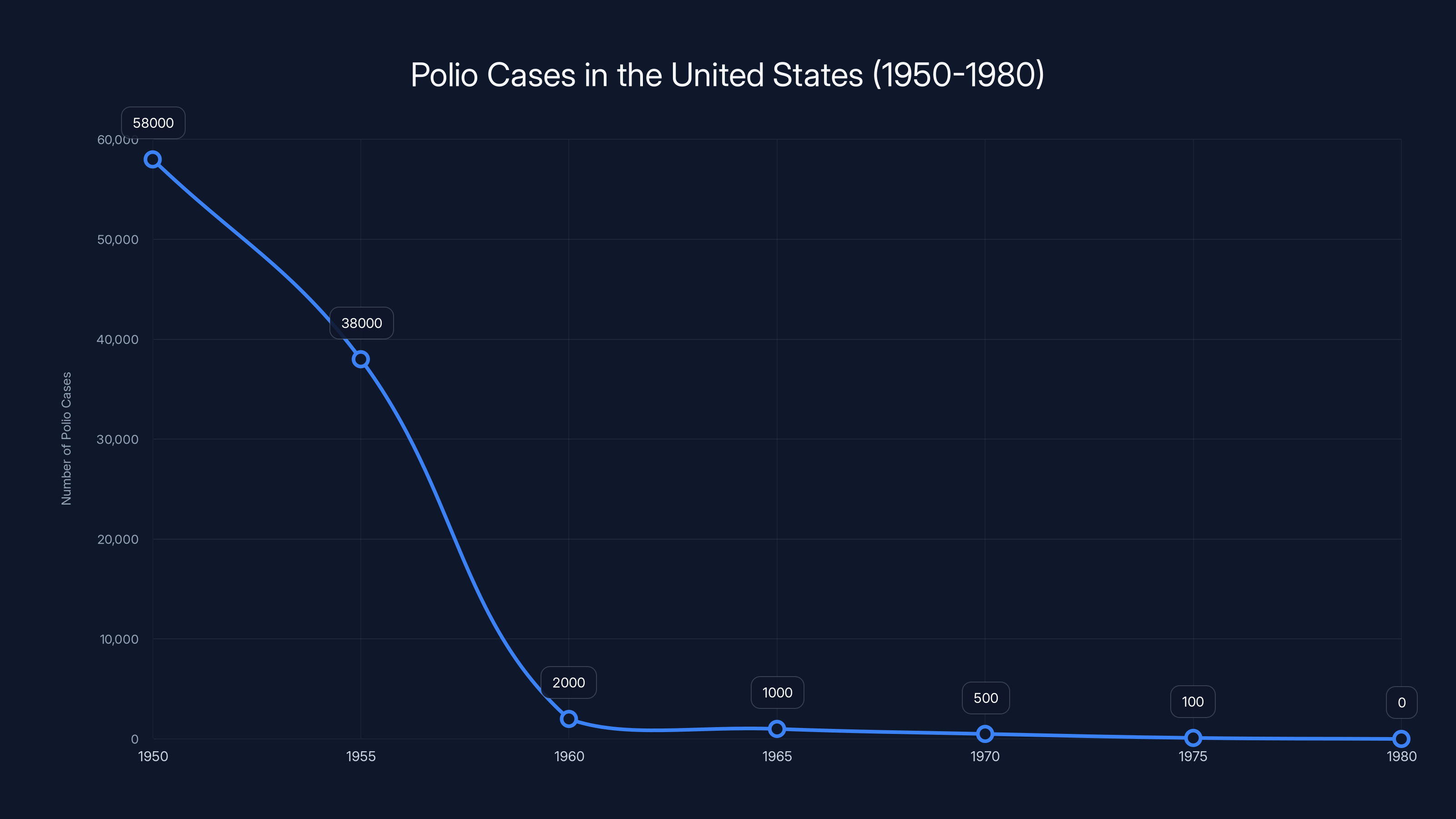
The introduction of the polio vaccine in 1955 led to a dramatic decline in polio cases, demonstrating the vaccine's critical role in disease elimination.
The Polio Question That Made Doctors Wince
But the moment that probably made the most cardiologists put their heads in their hands came when Milhoan questioned whether polio vaccines are even necessary today.
"I think also as you look at polio, we need to not be afraid to consider that we are in a different time now than we were then," he said, referring to the pre-vaccine era of the 1950s. He pointed to modern sanitation and suggested that disease risk has changed.
On the surface, this sounds reasonable. After all, he's technically correct that sanitation has improved. But this argument ignores a critical fact: polio doesn't care about your plumbing.
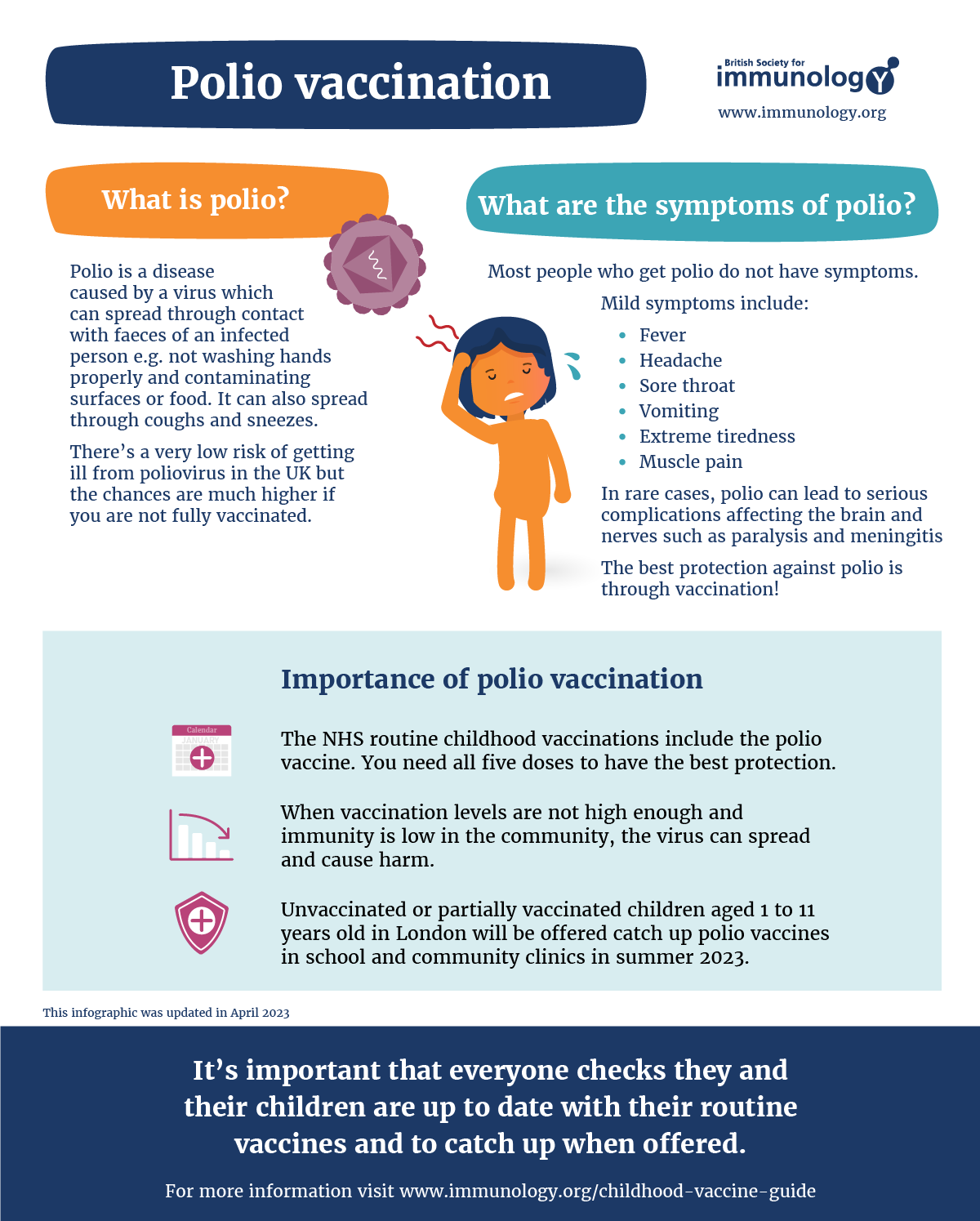
Polio is a viral disease. It spreads person-to-person through respiratory droplets and fecal-oral routes. Yes, better sanitation helps. But it doesn't create immunity. The only thing that stops polio is vaccination. This isn't speculation—it's documented medical history.
In the pre-vaccine era (before 1955), polio killed or paralyzed tens of thousands of Americans annually. In 1952 alone, there were over 58,000 reported cases and 3,145 deaths. Thousands more were left with permanent paralysis. Then the vaccine came, and those numbers dropped like a stone.
Today, the United States has zero endemic polio cases. Zero. Not because of sanitation alone, but because 95% of the population is vaccinated. This creates what epidemiologists call "herd immunity"—a threshold of immunity that stops the virus from spreading, even to the unvaccinated.
Millhoan wondered aloud: "If we take away all of the herd immunity, then does that switch, does that teeter-totter switch in a different direction?"
Yes. It does. That's not a theoretical question—that's how biology works.
Why This Matters: The Medical Community's Response
The American Medical Association didn't mince words. Sandra Adamson Fryhofer, AMA trustee, issued a statement that cut through the noise:
"This is not a theoretical debate—it is a dangerous step backward. Vaccines have saved millions of lives and virtually eliminated devastating diseases like polio in the United States. There is no cure for polio. When vaccination rates fall, paralysis, lifelong disability, and death return. The science on this is settled."
She was pointing out something crucial: Milhoan's framing as "individual autonomy" versus "population health" is a false choice. Moving away from routine immunizations doesn't increase freedom—it increases suffering.
Here's why: When vaccination rates drop below the herd immunity threshold (typically around 85-95% depending on the disease), the virus starts spreading again. It doesn't target only the unvaccinated. It spreads to newborns who can't yet be vaccinated, to immunocompromised people who can't mount an immune response, to people who had adverse reactions and can't receive boosters.
So when Milhoan talks about "freedom" to choose vaccination, what he's actually describing is the freedom for vulnerable people to get sick.

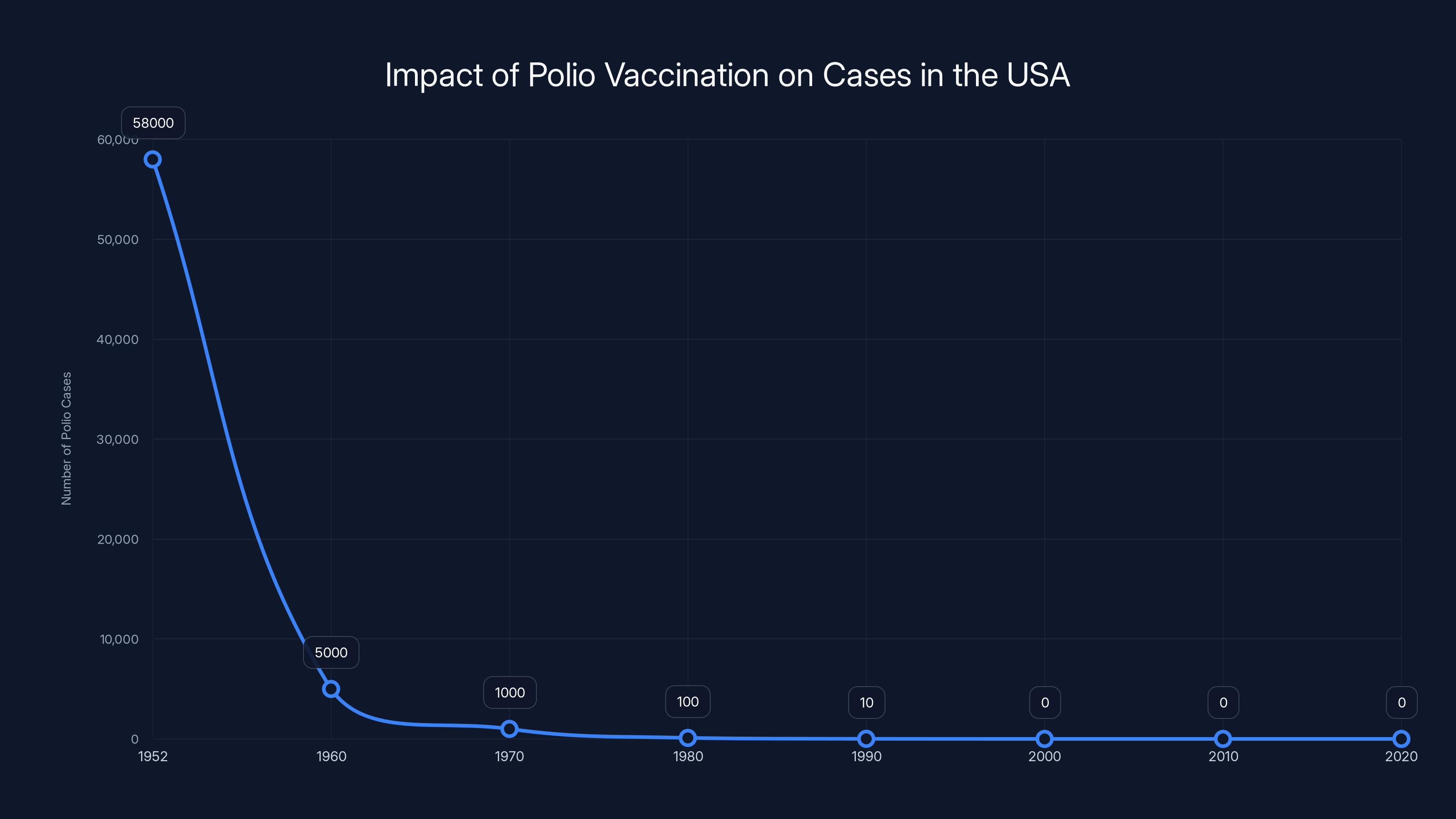
The introduction of the polio vaccine in the mid-1950s led to a dramatic decline in polio cases in the USA, showcasing the vaccine's critical role in disease control. Estimated data.
The Broader Context: Federal Vaccine Policy in Freefall
Millhoan's appointment didn't happen in a vacuum. Robert F. Kennedy Jr., now Health Secretary, has spent decades building a career on vaccine skepticism. His appointment marked a seismic shift in federal health policy.
According to analysis from the Kaiser Family Foundation, 27 states and Washington, DC, have already announced they will not follow current CDC vaccine recommendations. Instead, they're relying on older recommendations or their own state guidance.
This fragmentation is unprecedented. Before 2025, the CDC's immunization schedule was a national standard. Medical offices across the country followed it. Pharmacies stocked vaccines accordingly. Hospitals structured their protocols around it. It wasn't perfect, but it was coordinated.
Now? It's chaos.
The American Academy of Pediatrics announced its 2026 vaccine schedule as an explicit alternative to the CDC's recommendations, which the AAP said "depart from longstanding medical evidence and no longer offer the optimal way to prevent illnesses in children." That's diplomatic language for "the CDC is making dangerous recommendations."
Twelve other major medical organizations have endorsed the AAP's schedule, including the AMA, American Academy of Family Physicians, American College of Obstetricians and Gynecologists, Infectious Diseases Society of America, and Pediatric Infectious Diseases Society.
The medical establishment has effectively said: "We don't trust federal vaccine policy anymore. We're providing our own guidance."

Who Is Kirk Milhoan, Really?
Understanding how someone with Milhoan's views ended up chairing a federal vaccine advisory committee requires understanding the political landscape of vaccine skepticism.
Millhoan is a pediatric cardiologist. His specialty is the heart—not infectious disease, epidemiology, or immunology. Yet he's now guiding national vaccine policy.
This is like asking a dermatologist to chair the Federal Reserve. The credentials don't match the role.
What he brings to the table isn't expertise. It's ideology. His statements make clear he's part of the "I don't trust the scientific establishment" camp. This isn't because he's studied the evidence and found it wanting. It's because he's decided that personal observation trumps peer review.
That's not medicine. That's faith-based reasoning wearing a white coat.
The podcast interview revealed someone who:
- Makes false claims about vaccine safety
- Equates tiny risks with massive risks
- Questions the necessity of vaccines that eliminated deadly diseases
- Views vaccine skepticism as intellectual freedom rather than medical negligence
- Has been appointed to a position of significant power over federal health policy
This last point is crucial. Milhoan isn't just some random podcaster expressing his opinions. He chairs ACIP—the committee that shapes what the CDC recommends. When he questions whether polio vaccines are necessary, he's doing so from a position of authority.

The Historical Record on Polio: What Actually Happened
Let's look at what the data actually shows. Because if Milhoan's position has any merit, the historical record should support it.
Before the polio vaccine (pre-1955):
- Annual cases in the US: tens of thousands
- Annual deaths: thousands
- Annual paralysis cases: thousands
- Age distribution: primarily children under 14
After widespread vaccination (post-1960):
- Annual cases in the US: zero to single digits
- Annual deaths: zero
- Annual paralysis cases: zero
- Last endemic case in the US: 1979
That's not coincidence. That's causation. And it's been documented across every country that achieved high vaccination rates.
Globally, the World Health Organization estimates that polio vaccination has prevented 18 million deaths since 1988. That's not an estimate from vaccine manufacturers. That's from the international health organization that has no financial stake in vaccination.
Now, did sanitation improvements help? Absolutely. Better sanitation, clean water, and improved living conditions all contributed. But sanitation alone didn't eliminate polio. Countries with excellent sanitation that didn't vaccinate still saw polio cases. The vaccine was the deciding factor.
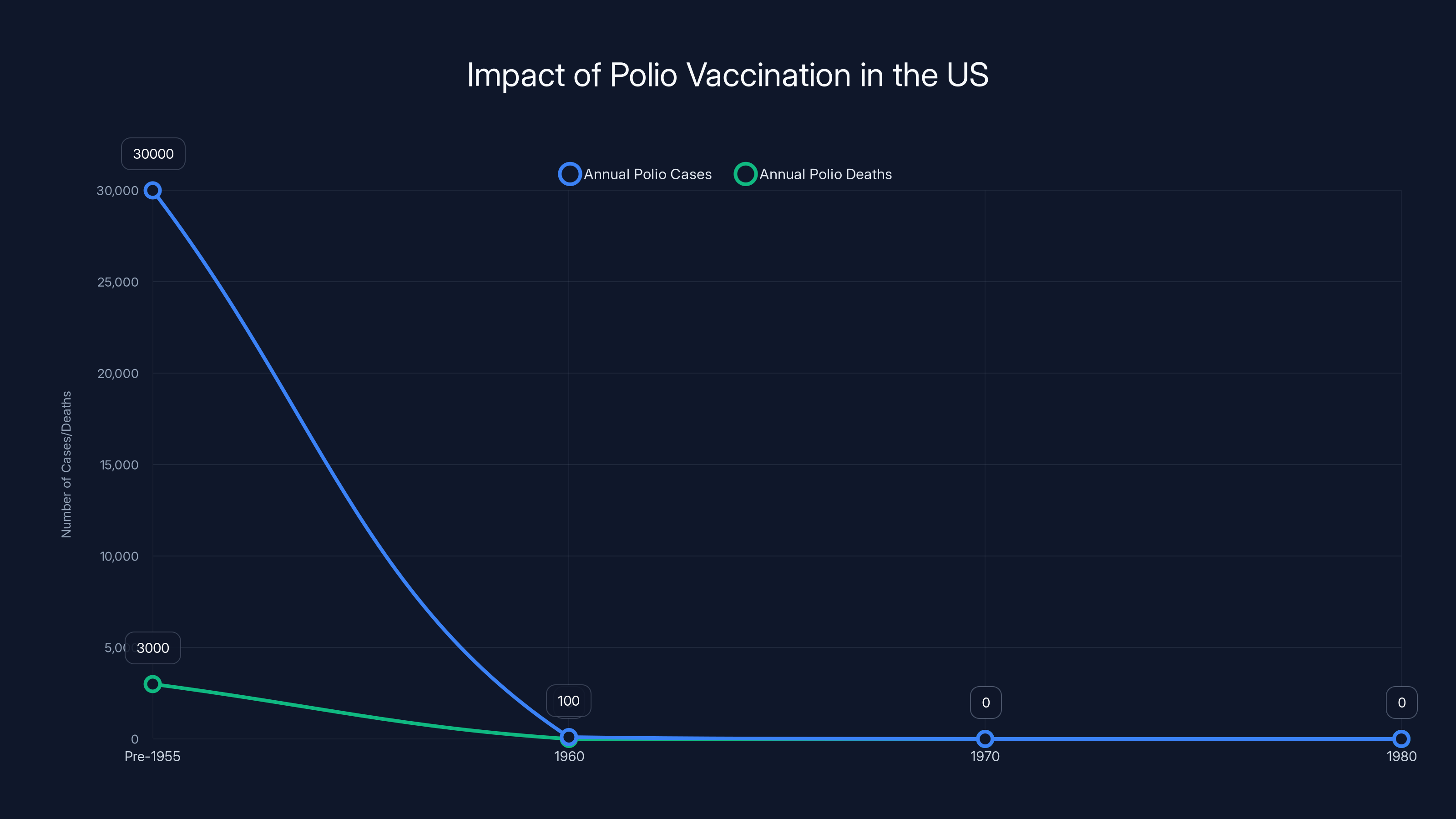
The introduction of the polio vaccine led to a dramatic decrease in both cases and deaths in the US, highlighting the vaccine's effectiveness. Estimated data based on historical trends.
The Risk Calculus: Disease vs. Vaccine
Millhoan claimed he was simply trying to weigh risks fairly. Let's actually do that calculation.
Polio, when it infects someone, has these risks:
- Asymptomatic infection: 70-75% of cases
- Minor symptoms (fever, sore throat): 24-25% of cases
- Non-paralytic aseptic meningitis: <1% of cases
- Paralysis: 1 in 200 infected children; 1 in 75 infected adults
- Death: 2-10% of paralyzed cases; rarely in asymptomatic cases
So if unvaccinated and infected, your risk of paralysis is 0.5-1.33%, and your risk of death if paralyzed is 2-10%.
The polio vaccine (inactivated polio vaccine, IPV):
- Serious allergic reactions: approximately 1 in 1 million doses
- Guillain-Barré syndrome (very rare): approximately 1-2 cases per million doses (though this rate is similar to the general population and may not be causally related)
- Most common side effects: soreness at injection site, low-grade fever
Now, the math:
Risk of paralysis from polio if unvaccinated and infected: 0.5-1.33%
Risk of serious harm from IPV: <0.0001%
That's a difference of approximately 5,000 to 13,300 times. The disease is thousands of times more dangerous than the vaccine.
Yet Milhoan spoke as if these risks were comparable. They're not. Not even close.
What Happened to ACIP?
The Advisory Committee on Immunization Practices used to be something different. It was a committee of vaccine experts—immunologists, epidemiologists, infectious disease specialists—who spent months reviewing evidence before making recommendations.
They had transparency. They had conflict-of-interest rules. They had a process.
Now? Milhoan chairs it, and he's already signaling that the evidence-based methodology that previous panels used is going to change. His dismissal of "established science" and insistence on personal observation suggests ACIP is about to become much more ideological and much less scientific.
This matters because ACIP recommendations shape what happens at the state level, what insurance covers, what pediatricians recommend to parents, and what public health messaging looks like.
When ACIP's credibility collapses, the entire system of vaccine guidance fragments. And when that happens, disease can return.
The Measles Warning Sign
We've actually seen what happens when vaccination rates drop. The measles outbreaks of 2019-2022 showed us exactly what we're risking.
Measles vaccination rates had dropped in certain communities due to vaccine skepticism. Result? In 2019, the US saw the largest measles outbreak in 27 years, with 1,282 cases and 7 deaths.
These weren't hypothetical cases. They were real people. Many were children too young to be vaccinated. Some were immunocompromised adults who couldn't be vaccinated.
We know what happens when Milhoan's philosophy gets implemented. We've seen it. And it results in sick children.
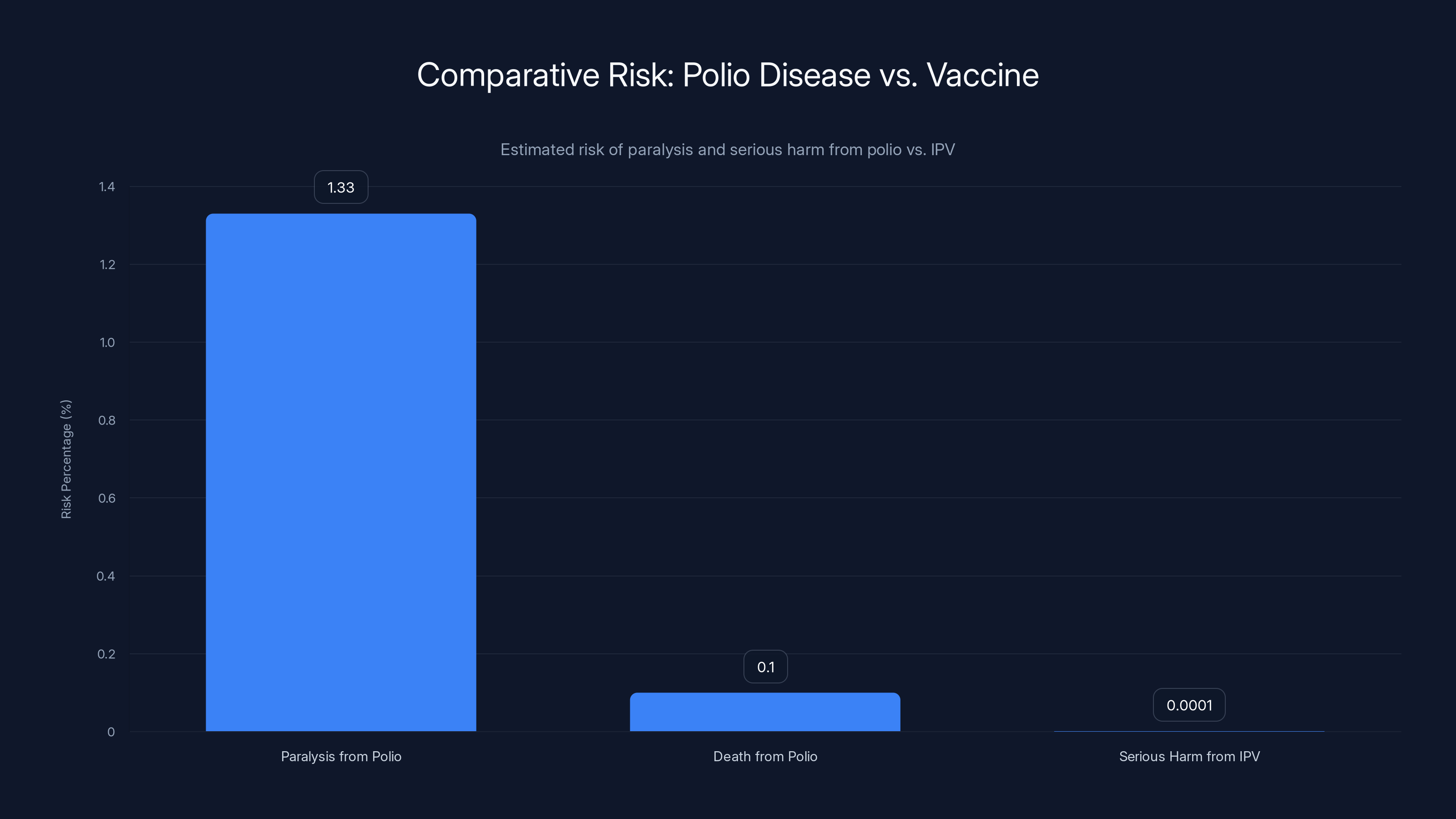
The risk of paralysis from polio is approximately 1.33%, while the risk of serious harm from the IPV vaccine is less than 0.0001%. The disease is thousands of times more dangerous than the vaccine.
The States' Response: Rejecting Federal Guidance
According to Kaiser Family Foundation analysis, the fracturing of vaccine policy is already underway:
- 27 states plus DC have announced they won't follow CDC recommendations
- States are looking to previous guidelines or their own state-level decisions
- Medical organizations are publishing alternative schedules
- Pediatricians are expressing confusion about what to recommend
This creates a patchwork system where vaccine recommendations depend on your zip code. A child in one state might be protected against diseases that another state's children are exposed to.
Public health doesn't work well with geographic fragmentation. Disease doesn't respect state borders.
Looking Forward: What Could Go Wrong
If current trends continue, here's what experts worry about:
- Vaccination rates dropping below herd immunity thresholds
- Diseases like measles, polio, and whooping cough returning to the United States
- Outbreaks affecting vulnerable populations: newborns, immunocompromised people, people who can't be vaccinated
- Healthcare systems becoming overwhelmed with preventable disease
- Economic costs from treating diseases that are now preventable (polio treatment costs approximately 10 per vaccine)
- Loss of trust in medical institutions generally
- Brain drain as experienced vaccine scientists and epidemiologists leave government service
None of this is inevitable. But it's the direction current policy is heading.

The Alternative: What Medical Consensus Actually Says
Meanwhile, the actual medical consensus has become clearer, not less. Twelve major medical organizations have endorsed a unified vaccine schedule that differs from the CDC's current guidance.
These aren't fringe organizations. They include:
- American Academy of Pediatrics
- American Medical Association
- American Academy of Family Physicians
- American College of Obstetricians and Gynecologists
- Infectious Diseases Society of America
- Pediatric Infectious Diseases Society
All of these groups have independently reviewed the evidence and concluded that the CDC's guidance under Kennedy-era leadership is problematic.
Their schedule is remarkably consistent with decades of previous practice. Nothing radical. Nothing new. Just maintaining the proven approach that's worked for decades.

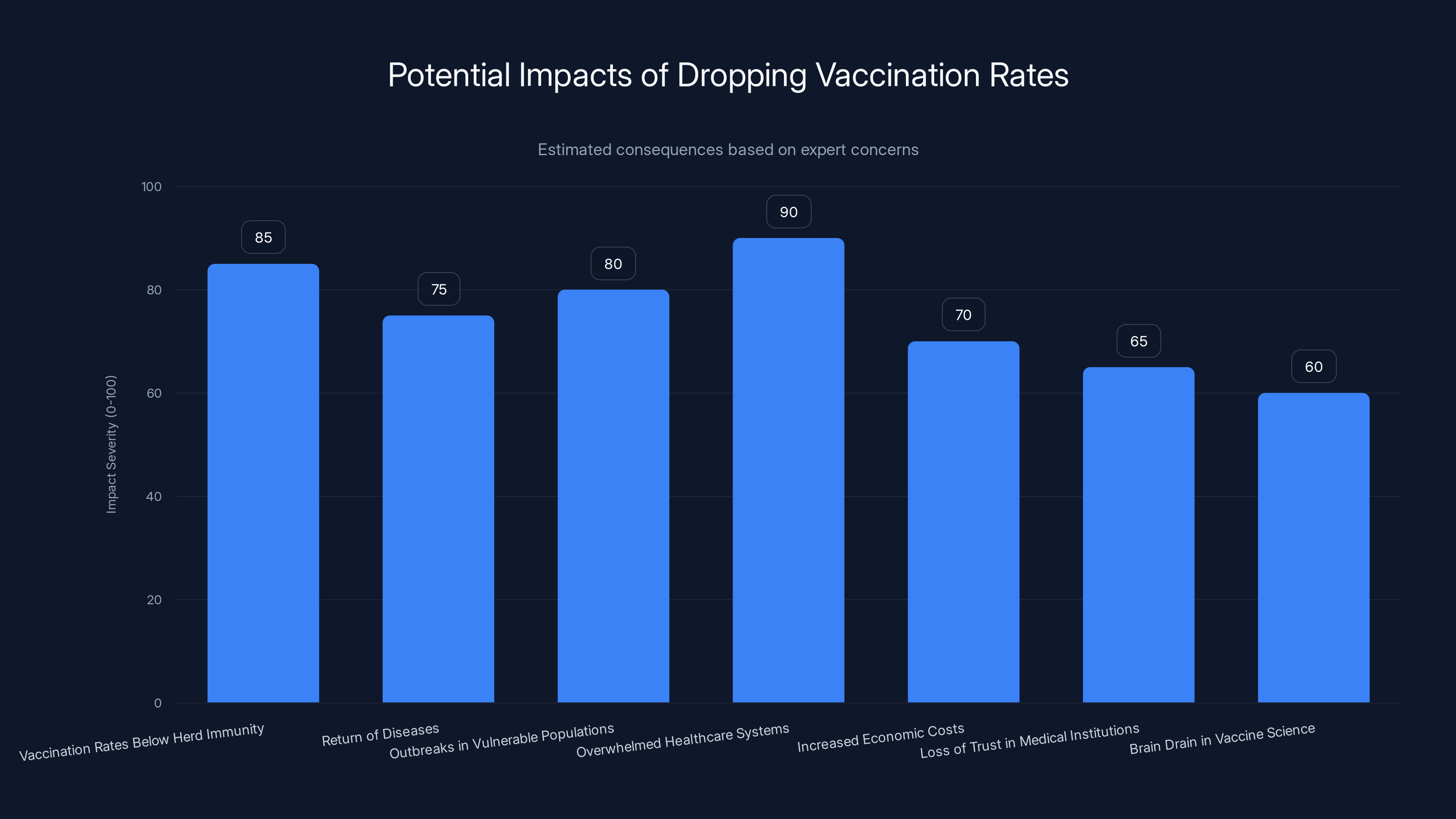
This chart estimates the severity of impacts if vaccination rates drop below herd immunity thresholds. The most significant concerns include overwhelmed healthcare systems and the return of preventable diseases. (Estimated data)
Public Health vs. Individual Choice: The False Dichotomy
Millhoan frames vaccine policy as a choice between "population health" and "individual autonomy." This is one of the most effective rhetorical moves of vaccine skeptics because it appeals to our values around freedom.
But it's a false choice.
Vaccines work through a collective action problem. If enough people are vaccinated, everyone benefits through herd immunity. If vaccination rates drop, everyone loses protection.
It's like asking whether we should prioritize "individual freedom to drive on any side of the road" versus "traffic safety." We've already solved that problem by deciding that coordinated behavior (staying on your side) benefits everyone, including the person who might prefer to drive on the left.
Vaccination is similar. Individual choice to not vaccinate imposes costs on others, particularly those who can't be vaccinated. That's not freedom—that's externalizing harm onto vulnerable people.

What This Means for Your Health Decision-Making
If you're reading this and feeling confused about what to believe, here's my honest assessment:
The medical consensus has spoken. Multiple independent medical organizations with expertise in infectious disease and immunology have reviewed the evidence and reached the same conclusion: polio vaccines are necessary, measles vaccines are necessary, and vaccines in general remain one of the most effective public health interventions ever created.
Kirk Milhoan's position is not supported by evidence. It's supported by ideology. There's a difference.
When making decisions about vaccination for yourself or your children, I'd suggest:
- Talk to your doctor (not the federal government right now)
- Look at what major medical organizations recommend (AAP, AMA, etc.)
- Ask your doctor about any specific concerns you have
- Remember that vaccine side effects are rare; vaccine-preventable diseases are far more dangerous
The fact that you have to do this investigation yourself is unfortunate. It shouldn't be necessary. But the credibility of federal vaccine policy has been compromised, and medical professionals have essentially said, "We'll handle this—don't trust the CDC." That's where we are.

The Bigger Picture: What Happens to Public Health When Trust Collapses
Millhoan's comments are emblematic of a larger problem: the erosion of expert institutions.
For decades, the CDC was the gold standard. Other countries envied our vaccine program. Parents trusted the recommendations. Pediatricians didn't have to choose between federal guidance and their own judgment.
Now that system is breaking. And what replaces it is messier, more fragmented, and ultimately less effective.
The scary part? This didn't happen because vaccine science changed. The evidence for vaccine safety and effectiveness is stronger than ever. This happened because political ideology entered the room.
When someone becomes Health Secretary specifically because they don't believe in vaccines, and then appoints vaccine skeptics to positions where they oversee vaccine policy, you don't get better policy. You get ideology masquerading as science.
That's what Milhoan represents. Not rigorous skepticism. Not careful evidence review. Just a different set of beliefs presented with the authority of a government position.

Conclusion: This Is About Real People
All of this might seem abstract—debates about herd immunity thresholds, federal policy, institutional trust. But Milhoan's comments have concrete implications.
If vaccination rates drop, real children will get paralyzed by polio. Real infants will get measles. Real people will die from preventable diseases.
That's not theoretical. That's what the historical record shows happens when vaccine skepticism becomes policy.
The good news is that the medical community hasn't abandoned ship. Major medical organizations have published alternative guidance. Pediatricians are ignoring the federal guidance and following their professional judgment. States are making their own decisions.
In the short term, this fragmentation is messy. But it may prevent the worst outcomes.
The challenge is that this isn't sustainable long-term. You can't run a public health system where different states have different vaccine schedules. You can't expect patients to navigate conflicting guidance. And you can't expect healthcare professionals to keep questioning decisions that used to be settled.
Eventually, one of two things happens: either federal vaccine policy gets corrected and expert institutions regain credibility, or disease returns and reminds us why vaccines matter.
I'm hoping for option one. But Milhoan's appointment and his comments suggest we might be heading toward option two.
FAQ
What makes Kirk Milhoan's comments about polio vaccines so controversial?
Millhoan questioned whether polio vaccines are necessary today, citing improved sanitation and lower disease risk. Medical experts found this dangerous because polio is a viral disease that requires vaccination for immunity—not just sanitation. His comments represent a fundamental misunderstanding of how polio spreads and how vaccines work, combined with a concerning pattern of downplaying vaccine risks while exaggerating disease eradication from factors other than vaccines.
Why did the American Medical Association feel compelled to respond?
The AMA responded because Milhoan chairs a federal committee that shapes vaccine policy, making his false claims potentially influential. He falsely linked vaccines to allergies and asthma, claimed COVID vaccines killed children without evidence, and equated tiny vaccine risks with massive disease risks. The AMA recognized this posed a direct threat to public health guidance and felt obligated to publicly correct the record.
How did we actually eliminate polio in the United States?
Polio was eliminated through widespread vaccination starting in 1955 when the inactivated polio vaccine became available. Before the vaccine, polio caused 58,000 cases annually in the US and thousands of deaths and paralyses. After vaccination rates exceeded the herd immunity threshold (85-95%), transmission stopped completely. The last endemic polio case in the United States occurred in 1979. Sanitation improvements helped, but vaccination was the deciding factor—countries with good sanitation but low vaccination rates still experienced polio outbreaks.
What is herd immunity and why does it matter for diseases like polio?
Herd immunity occurs when enough of a population is immune to a disease (through vaccination or prior infection) that transmission stops. For polio, this threshold is approximately 85-95%. When vaccination rates fall below this threshold, the virus can spread again, including to people who cannot be vaccinated (newborns, immunocompromised people). When Milhoan suggested we "take away all herd immunity," he was describing a scenario where vulnerable people would become exposed to a deadly disease.
How do vaccine risks compare to disease risks for polio?
The inactivated polio vaccine (IPV) causes serious allergic reactions in approximately 1 in 1 million doses. Polio infection causes paralysis in 1 in 200 infected children and 1 in 75 infected adults. Death from polio paralysis occurs in 2-10% of paralyzed cases. This means polio is approximately 5,000 to 13,300 times more dangerous than the vaccine. The risks are not comparable—they differ by orders of magnitude.
Why are 27 states rejecting CDC vaccine recommendations?
Following Robert F. Kennedy Jr.'s appointment as Health Secretary and his overhaul of CDC vaccine recommendations, numerous states and major medical organizations (AAP, AMA, IDSA) concluded the new federal guidance "departs from longstanding medical evidence." Rather than follow federal recommendations, states and medical professionals are relying on previous CDC guidance or their own state-level recommendations. This fragmentation reflects loss of confidence in federal vaccine policy rather than any change in the science underlying vaccine effectiveness.
What happened to polio vaccination rates when skepticism increased?
In Afghanistan and Pakistan, political instability combined with vaccine skepticism caused vaccination rates to drop, and polio never achieved eradication. These two countries remain the only places where polio still circulates endemically. This demonstrates what happens globally when vaccination rates fall below herd immunity thresholds—the disease persists, and outbreaks continue. It's a real-world example of the scenario Milhoan was hypothetically questioning.
Should I trust federal vaccine guidance or medical organizations instead?
Given current circumstances, major medical organizations (American Academy of Pediatrics, American Medical Association, Infectious Diseases Society of America) have published alternative guidance based on their review of the same evidence. These organizations have reputational incentives to be correct and update their recommendations based on evidence. Your pediatrician's judgment, informed by their professional organization's guidance, is likely more reliable than federal guidance during this period of institutional uncertainty.
What was the 2019 measles outbreak, and what does it tell us about vaccination rates?
The 2019 measles outbreak, the largest since 1992, resulted in 1,282 cases and 7 deaths when vaccination rates dropped in certain communities due to vaccine skepticism. The outbreak affected infants too young to be vaccinated and immunocompromised people unable to be vaccinated. This is the real-world consequence of declining vaccination rates and exactly what experts worry will happen with polio and other preventable diseases if Milhoan's skepticism influences policy and vaccination rates drop.
How much does it cost to prevent polio versus treat paralysis?
A course of polio vaccine costs approximately

Key Takeaways
Polio vaccination doesn't depend on sanitation improvements alone—viral immunity from vaccination is essential. Milhoan's position that vaccine risks equal disease risks misrepresents the evidence by orders of magnitude. Federal vaccine policy has lost credibility with medical organizations, who now publish alternative guidance. Medical consensus remains unchanged: vaccines are safe and necessary. When vaccination rates fall below herd immunity thresholds, vulnerable populations (newborns, immunocompromised people) lose protection. The 2019 measles outbreak showed exactly what happens when vaccination rates decline due to skepticism.


