![Keto Rash Explained: Why Ketosis Causes Prurigo Pigmentosa [2025]](https://tryrunable.com/blog/keto-rash-explained-why-ketosis-causes-prurigo-pigmentosa-20/image-1-1769258180937.jpg)
Introduction: The Unexpected Side Effect Nobody Talks About
You've probably heard about the keto flu. Nausea, fatigue, brain fog during the first two weeks of cutting carbs. That's well documented. But there's another side effect that catches people off guard because it's rarely mentioned in fitness forums or diet guides.
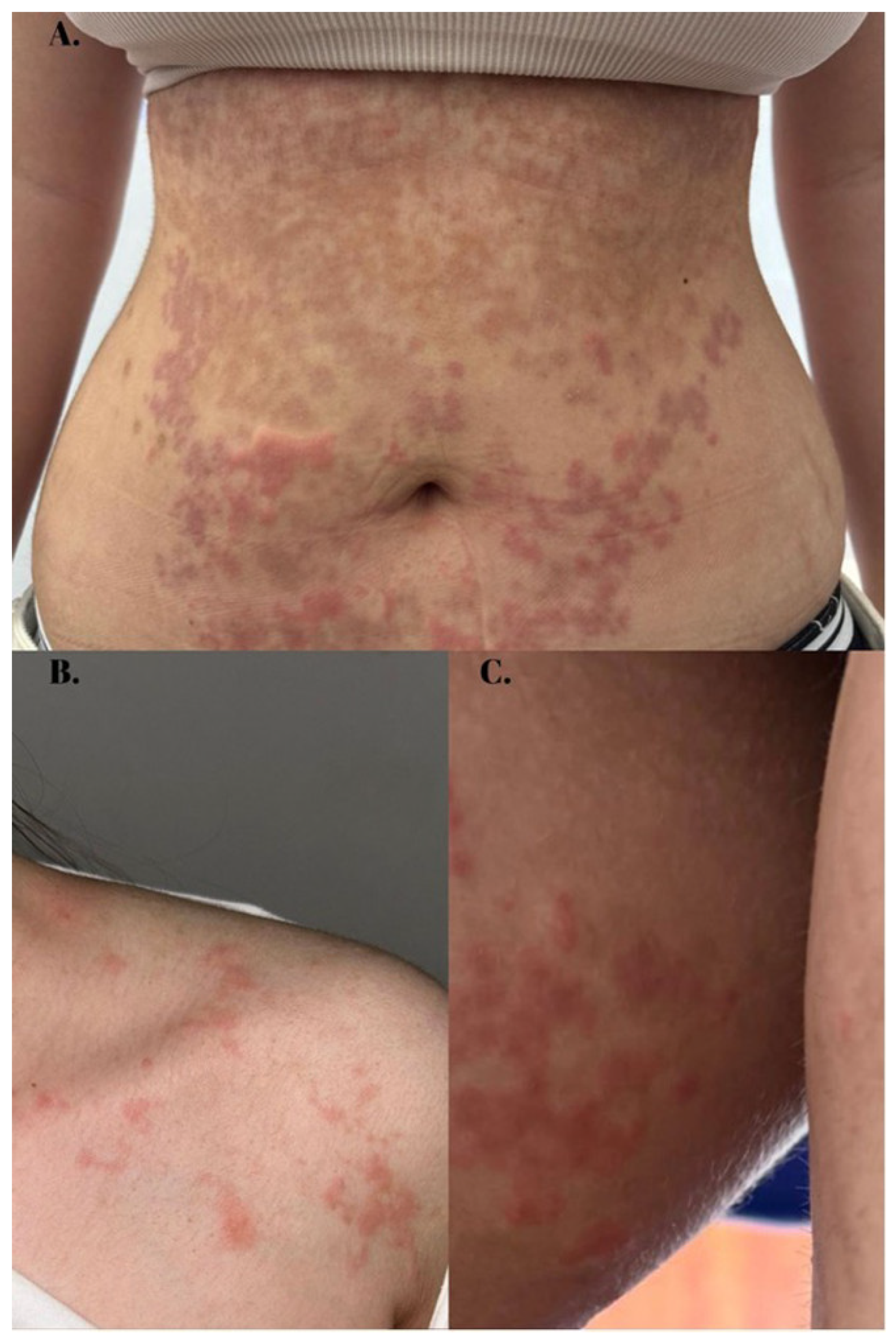
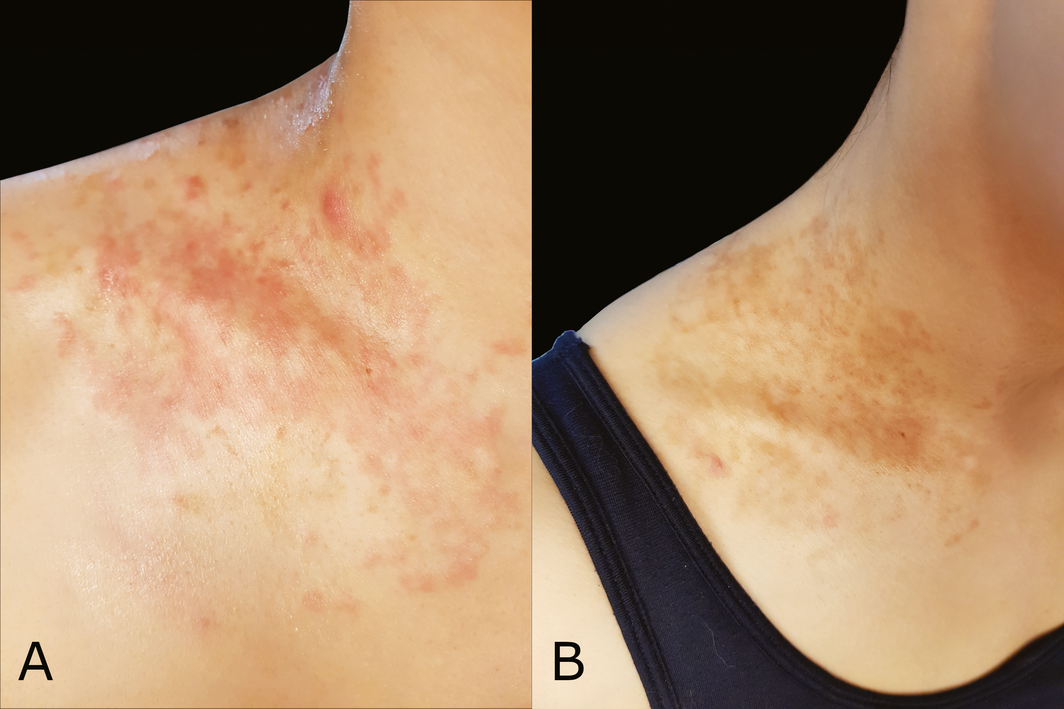
It's a rash. Not just any rash, but a specific condition called prurigo pigmentosa that appears as raised, red, itchy bumps typically across the chest, shoulders, and back. Some people develop patches of darkened skin interlaced with the inflammation. It shows up weeks into ketosis, persists stubbornly, and vanishes almost instantly once you stop the diet.
The frustrating part? Scientists still don't fully understand why it happens.
A 20-year-old man in Taiwan experienced exactly this. He switched to keto, lost some weight, felt good about his metabolic shift. Then his chest and shoulders erupted into an angry rash that wouldn't go away. A dermatologist's biopsy showed swelling between skin cells and inflammation around blood vessels, but standard allergy and infection tests came back negative. The diagnosis only clicked when the doctors asked about his diet. Two months into ketosis, his body was literally rebelling against the metabolic state he'd induced.
This case, published in a major medical journal, represents hundreds of documented incidents. The rash has been linked to ketogenic diets, extended fasting, post-bariatric surgery weight loss, and even diabetes. Yet the mechanism remains elusive. Researchers have hypotheses. They know ketone levels correlate with outbreak severity. But the exact biological pathway that transforms harmless ketone bodies into an inflammatory skin condition? That's still a mystery.
Here's what we know about keto rash, why it happens, how to recognize it, and what actually works to make it disappear.
TL; DR
- Prurigo pigmentosa is a documented skin condition linked to ketosis with confirmed cases but unknown underlying mechanisms
- The rash typically appears 3-6 weeks into ketosis on the chest, shoulders, and back as raised red bumps that itch intensely
- Neutrophil-driven inflammation is the leading hypothesis, but researchers still debate the exact trigger
- Tetracycline antibiotics (especially doxycycline) are highly effective, eliminating symptoms within 7-14 days
- Exiting ketosis provides relief within days, though some people successfully continue keto with preventive measures

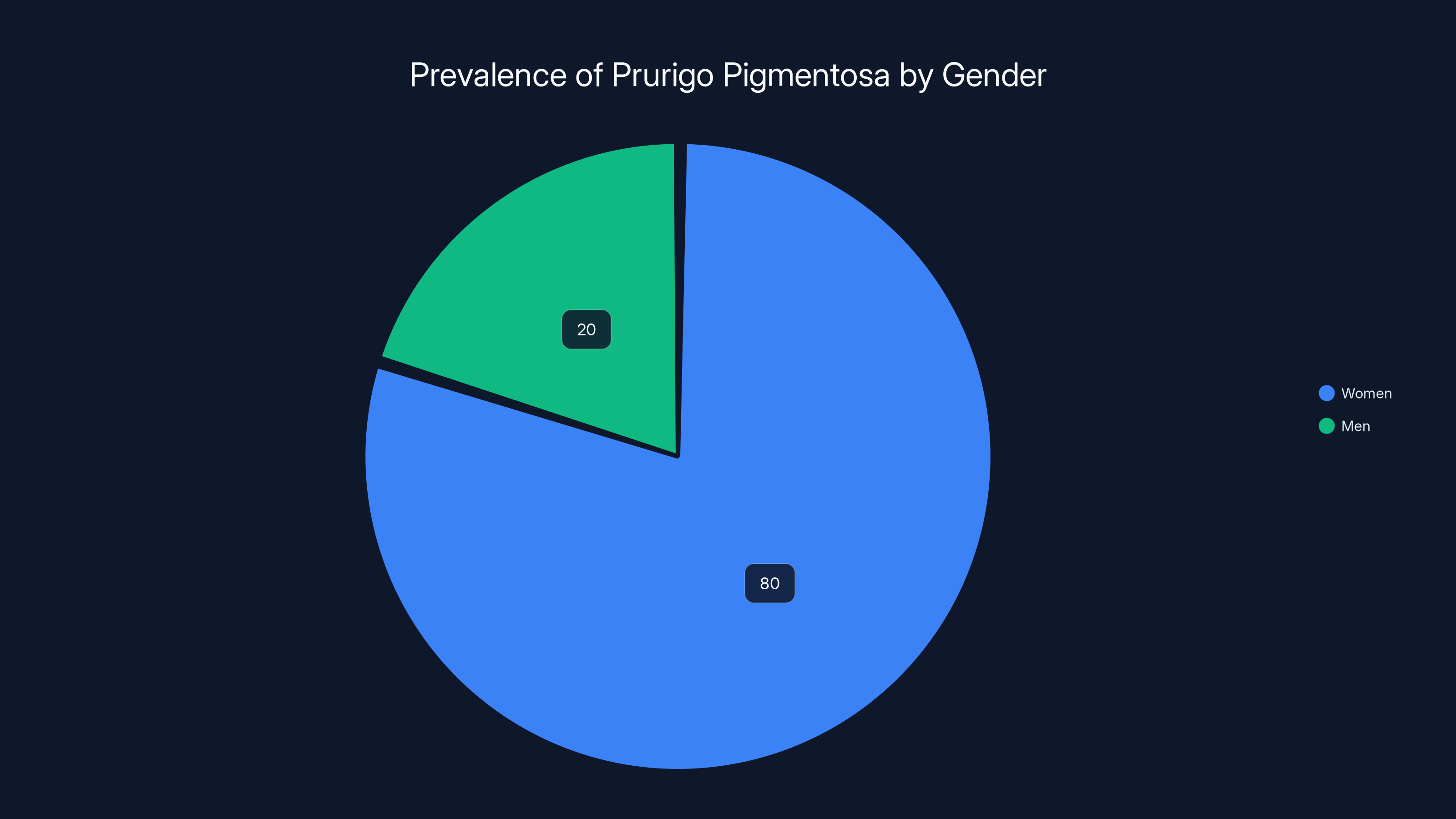
Prurigo pigmentosa was initially observed predominantly in women, with an estimated 80% of cases, compared to 20% in men. Estimated data.
What Is Prurigo Pigmentosa and Why Does It Matter
Prurigo pigmentosa isn't new. Japanese dermatologists first identified and named the condition in 1971. Back then, it appeared almost exclusively in women, which led researchers initially to wonder if hormonal factors were involved. They're not, as later cases would demonstrate.
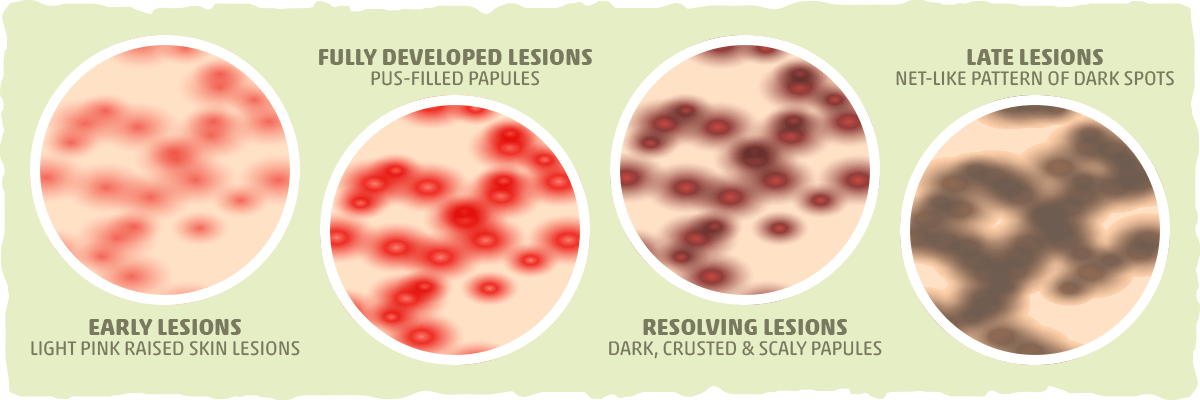
The name itself is descriptive. Prurigo means itchy, and pigmentosa refers to the pigmentation changes that develop alongside the inflammation. The condition presents in waves. Early stage shows isolated red bumps that feel raised and inflamed. They cluster around the chest, shoulders, neck, and upper back. The itching is intense enough that people scratch, which can lead to secondary infections and scarring.
As it progresses, the inflammatory lesions remain, but the skin surrounding them develops hyperpigmentation. This creates a striking visual pattern: red, inflamed bumps surrounded by darkened skin. This two-tone appearance is actually diagnostic. It's unusual enough that a dermatologist who's seen prurigo pigmentosa before will recognize it immediately.
The condition is benign in the sense that it doesn't threaten life or cause systemic illness. But it's far from minor. The itching disrupts sleep. The appearance creates embarrassment, especially when the rash spreads to visible areas. People describe it as unbearable, driving them to seek medical help urgently.
What makes prurigo pigmentosa particularly frustrating is its specificity to metabolic states. It doesn't appear in people eating normal carbohydrate-based diets. It doesn't show up in standard allergic or infectious skin conditions. It's almost exclusively linked to ketosis, which means it's a metabolic phenomenon masquerading as a dermatological one.
This connection also means the condition was essentially invisible to medicine for decades. Ketogenic diets were rarely prescribed except for specific neurological conditions. Most dermatologists trained before the 2010s never encountered prurigo pigmentosa. As low-carb dieting exploded in popularity, the condition suddenly appeared in clinics more frequently, yet the medical literature remained sparse.
The first major modern case series came in 2014 when a Japanese researcher reviewed 62 cases of prurigo pigmentosa linked to ketosis and fasting. By then, dermatologists were starting to see patterns. The condition appeared consistently. It responded to specific treatments. It correlated with metabolic markers. Yet why it happened remained theoretical.
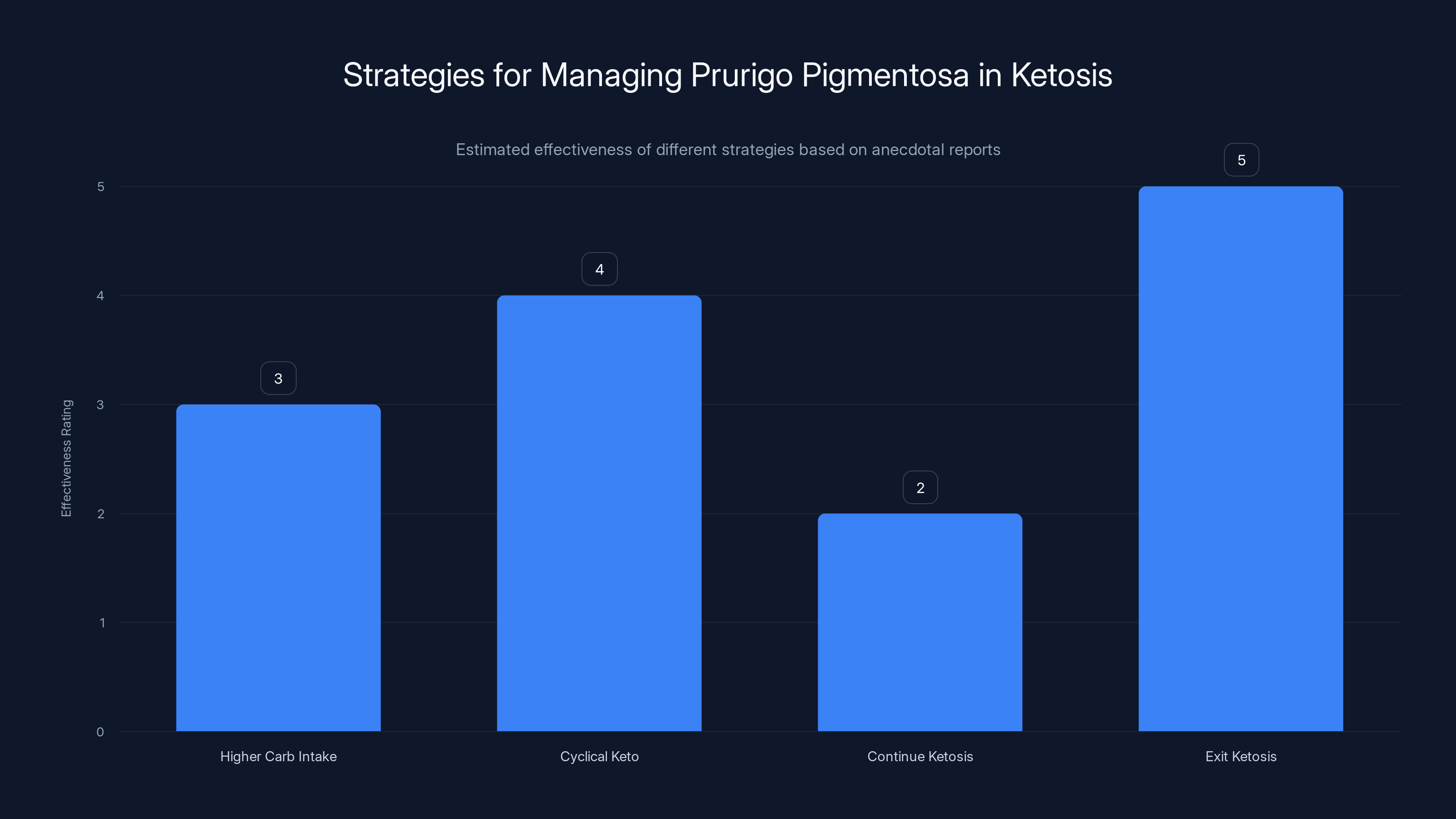
Exiting ketosis is reported as the most effective strategy to resolve prurigo pigmentosa, while cyclical keto shows promise with moderate effectiveness. Estimated data based on anecdotal evidence.
The Biochemistry of Ketosis: Understanding the Metabolic Shift
To understand why ketosis might trigger inflammation, you need to understand what ketosis actually is. It's not a dangerous state despite what some medical professionals claim. It's a normal, metabolic process that your body enters when carbohydrate availability drops below a certain threshold.
When you eat carbohydrates, your body breaks them down into glucose. This glucose enters your bloodstream, triggering insulin release, which shuttles the glucose into cells for immediate energy or storage. Your cells are happy. Your brain gets glucose. Your muscles get glucose. Everything runs on the preferred fuel source.
When carbohydrate intake drops dramatically, glucose production slows. Your body's glycogen stores deplete within 24-48 hours depending on activity level and initial storage capacity. At this point, your cells need energy but glucose isn't available. Your body initiates a metabolic shift.
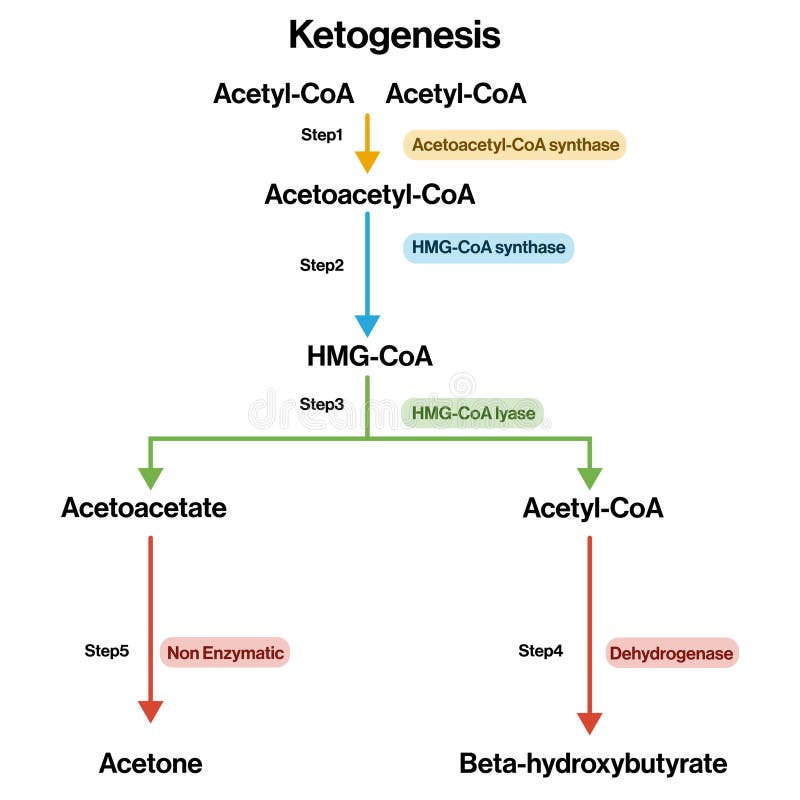
Lipolysis begins. Fat tissue releases free fatty acids into the bloodstream. These fatty acids travel to the liver, where they undergo beta-oxidation. This process breaks fatty acid chains into a two-carbon molecule called acetyl-Co A. Normally, acetyl-Co A enters the citric acid cycle to generate ATP (cellular energy). But when fat burning is extremely high, acetyl-Co A production exceeds the citric acid cycle's capacity to process it.
The excess acetyl-Co A takes an alternative route. The liver converts it into ketone bodies through a process called ketogenesis. Three primary ketones form: acetoacetate, beta-hydroxybutyrate, and acetone. Of these, beta-hydroxybutyrate and acetoacetate are metabolically active. Acetone is essentially a waste product that you exhale (hence keto breath).
The chemistry is straightforward: Ketone bodies = excess acetyl-Co A that the liver converts into alternative fuel molecules.
Ketone bodies enter the bloodstream and distribute throughout the body. Tissues that rely heavily on energy, especially the brain, readily use ketones as fuel. Your brain can derive up to 70 percent of its energy from ketones during extended ketosis. Muscles, heart, and kidneys also use ketones efficiently.
This metabolic state is neither inherently healthy nor unhealthy. It's simply different from the carbohydrate-fed state. Your ancestors entered ketosis regularly during times of food scarcity. Your body has elegant mechanisms to manage it. The concern only arises when ketone accumulation becomes extreme, as happens in diabetic ketoacidosis, a medical emergency where ketone blood levels become toxic.
For most people following a ketogenic diet, blood ketone levels range from 0.5 to 3 millimoles per liter. This is well below dangerous levels. Yet even at these mild-to-moderate ketone concentrations, some people develop prurigo pigmentosa.
Here's where the mystery deepens. Not everyone in ketosis develops the rash. Estimates suggest 1-3 percent of people following ketogenic diets experience it. Women may have slightly higher rates, though more recent data challenges the gender disparity seen in early Japanese cases. Some people ketone-fast for years without any rash. Others develop it within weeks. The individual variation is striking, which suggests genetic factors, inflammatory predisposition, or other metabolic variables play roles that researchers haven't yet identified.
The Immune Response Theory: Neutrophils and Inflammation
The leading hypothesis about prurigo pigmentosa focuses on immune activation. Specifically, it implicates a type of white blood cell called a neutrophil and the inflammatory cascade it triggers.
Neutrophils are front-line defenders. They're the most abundant white blood cell, making up about 50-70 percent of circulating leukocytes. When your body detects a threat—an infection, injury, or inflammatory signal—neutrophils mobilize rapidly. They squeeze through blood vessel walls into tissue, migrate toward the threat, and attack. They kill bacteria, engulf foreign particles, and release inflammatory chemicals.
Under a microscope, skin biopsies from people with prurigo pigmentosa show exactly this pattern: swelling between skin cells, inflammation around blood vessels, and neutrophil infiltration. It looks like your skin is fighting an infection, except cultures come back negative. There's no bacteria, no virus, no fungus. Your immune system is reacting to something, but it's not a pathogenic invader.
So what triggers the neutrophils? The current hypothesis is that elevated ketone bodies themselves, or the metabolic byproducts accompanying ketosis, activate inflammatory pathways. Ketones are acidic. When they accumulate in high concentrations, they lower blood p H slightly. This acidosis might trigger innate immune sensors that normally respond to metabolic stress or pathogenic signals.
Specifically, researchers point to pattern recognition receptors on immune cells that respond to metabolic danger signals. When your body is in a state of stress, these receptors activate. Ketosis might be perceived as metabolic stress even though it's functionally normal. This activates the inflammasome, a complex of proteins that orchestrates inflammatory responses.
The inflammasome triggers release of inflammatory cytokines, particularly interleukin-1 (IL-1) and tumor necrosis factor (TNF). These are signaling molecules that tell other immune cells to activate. Neutrophils receive the signal and rush to affected tissues. In the skin around blood vessels in areas prone to friction or thermal stress, they accumulate. The inflammation manifests as the raised, red rash.
But this remains a hypothesis. It explains the observed inflammation but doesn't explain why ketones trigger it in some people and not others. It doesn't explain the hyperpigmentation phase. And it doesn't fully account for why identical ketone blood levels cause rashes in some individuals while others at the same metabolic state remain unaffected.
Some researchers propose additional mechanisms. Ketosis might alter the microbiome in ways that trigger immune activation. Changes in skin barrier function during ketosis might increase susceptibility. Hormonal shifts accompanying both ketosis and weight loss might modify immune responsiveness. The truth likely involves multiple overlapping factors, not a single trigger.
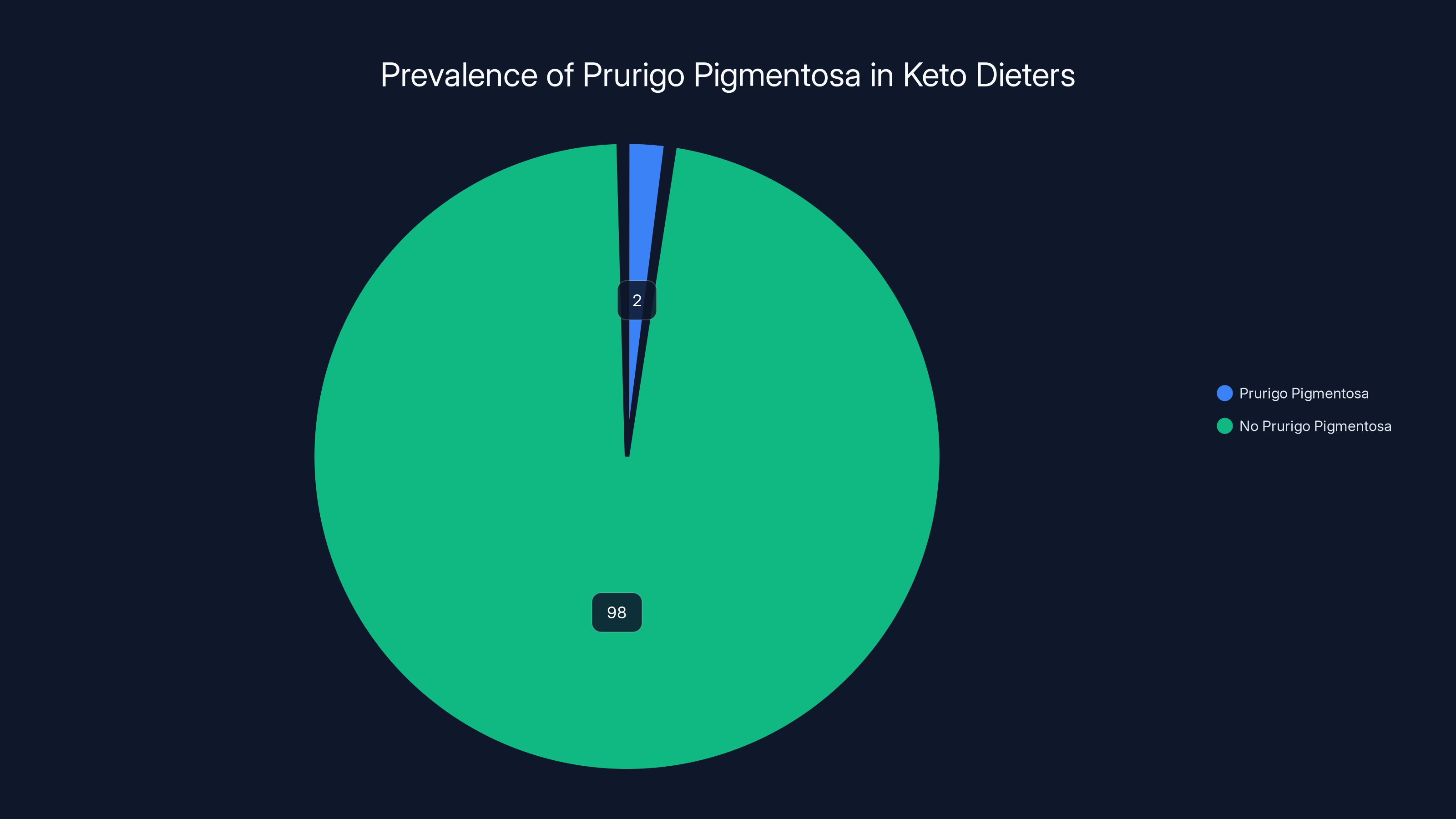
An estimated 1-3% of people on ketogenic diets develop prurigo pigmentosa, highlighting its rarity but potential impact given the diet's popularity. Estimated data.
Clinical Presentation: Recognizing the Rash
If you're considering ketosis or already following a ketogenic diet, knowing what to look for is critical. Prurigo pigmentosa has a distinctive presentation that helps differentiate it from other skin conditions.
The rash typically appears 3-12 weeks into ketosis, though cases as early as two weeks and as late as several months exist. The presentation often starts with a few isolated lesions that spread over days or weeks. The bumps are raised, usually 2-5 millimeters in diameter. They're firm, not soft or pustular. The surrounding skin is red and inflamed.
The itching is intense. People describe it as unbearable, sometimes disturbing sleep. Scratching provides temporary relief but causes additional irritation and risk of secondary bacterial infection.
Anatatomically, the rash favors the chest, shoulders, and upper back. This distribution pattern is so consistent that it's considered diagnostic. The neck and upper arms may be involved, but the face, hands, feet, and lower legs are typically spared. The rash rarely appears on the abdomen or thighs.
As the rash persists over weeks, the inflammatory lesions remain but the surrounding skin develops hyperpigmentation. The darkened skin creates the characteristic appearance: red, raised bumps surrounded by brown or tan discoloration. This pattern is quite striking and distinct from other inflammatory skin conditions.
In some cases, the inflammation resolves but the hyperpigmentation persists for months. This can be psychologically challenging even after the itching stops, because the visual appearance remains.
The rash doesn't respond to standard treatments for other common skin conditions. Topical steroids provide minimal relief. Antihistamines don't help because it's not an allergic reaction. Antifungal creams are useless because there's no fungal infection. This lack of response to standard treatments often frustrates patients and drives them to seek specialist evaluation.
Differential diagnosis is important. Other conditions that might present similarly include:
Atopic dermatitis: Causes intense itching and inflammation but typically has a different distribution and history. It usually appears in skin folds and areas of friction, not specifically the chest and shoulders.
Contact dermatitis: Results from exposure to irritating substances. The distribution would be random based on contact points, not localized to chest and shoulders.
Bacterial or fungal infection: Shows pustules, drainage, or scaling. Cultures would be positive.
Polymorphous light eruption: Sun-triggered, worse on exposed areas like the face and arms. Prurigo pigmentosa shows no association with sun exposure.
Pityriasis rosea: A viral rash that appears on the trunk but follows a specific pattern with a herald patch. Prurigo pigmentosa lacks this pattern.
A dermatologist experienced with metabolic conditions will recognize prurigo pigmentosa by its appearance and distribution, especially combined with a history of recent ketosis initiation. Confirmation can come from a skin biopsy showing the characteristic histopathology: spongiosis (swelling between skin cells), perivascular inflammation (inflammation around blood vessels), and neutrophilic infiltration (abundance of neutrophil immune cells).

Documented Cases: Real-World Evidence
The medical literature documents dozens of confirmed cases of prurigo pigmentosa linked to ketogenic diets. Each case adds nuance to understanding who develops the rash and under what circumstances.
The 2014 Japanese case series reviewed 62 patients with prurigo pigmentosa. Of these, 47 were associated with fasting or low-carbohydrate diets. The remaining 15 occurred in people with diabetes or following bariatric surgery. This distribution is telling: the rash appears specifically in conditions inducing ketosis or metabolic disruption, not across a broad spectrum of skin conditions.
Gender split in that series showed women comprising 71 percent of cases, but more recent case reports show a more balanced gender distribution, suggesting the earlier gender bias reflected reporting patterns or differences in healthcare-seeking behavior rather than true biological differences.
Age range spans from late teens through elderly individuals, with most cases appearing in adults aged 20-55. Young people experimenting with trendy diets and older individuals attempting weight loss for health reasons both experience the rash.
Weight loss magnitude varies. Some people with minimal weight loss develop the rash; others lose 30+ percent of body weight without it. This suggests weight loss alone doesn't trigger the rash—the metabolic state of ketosis is what matters.
Severity varies dramatically. Some cases involve a few scattered lesions that cause mild itching. Others present with extensive rashes covering large portions of the trunk, causing significant discomfort and psychological distress. The factors determining severity remain unclear, though inflammatory predisposition and genetic factors likely contribute.
A particularly interesting subset involves people who develop prurigo pigmentosa specifically during fasting windows in intermittent fasting protocols. This demonstrates that the rash isn't specific to strict ketogenic diets; it appears whenever metabolic conditions favor sustained ketosis.

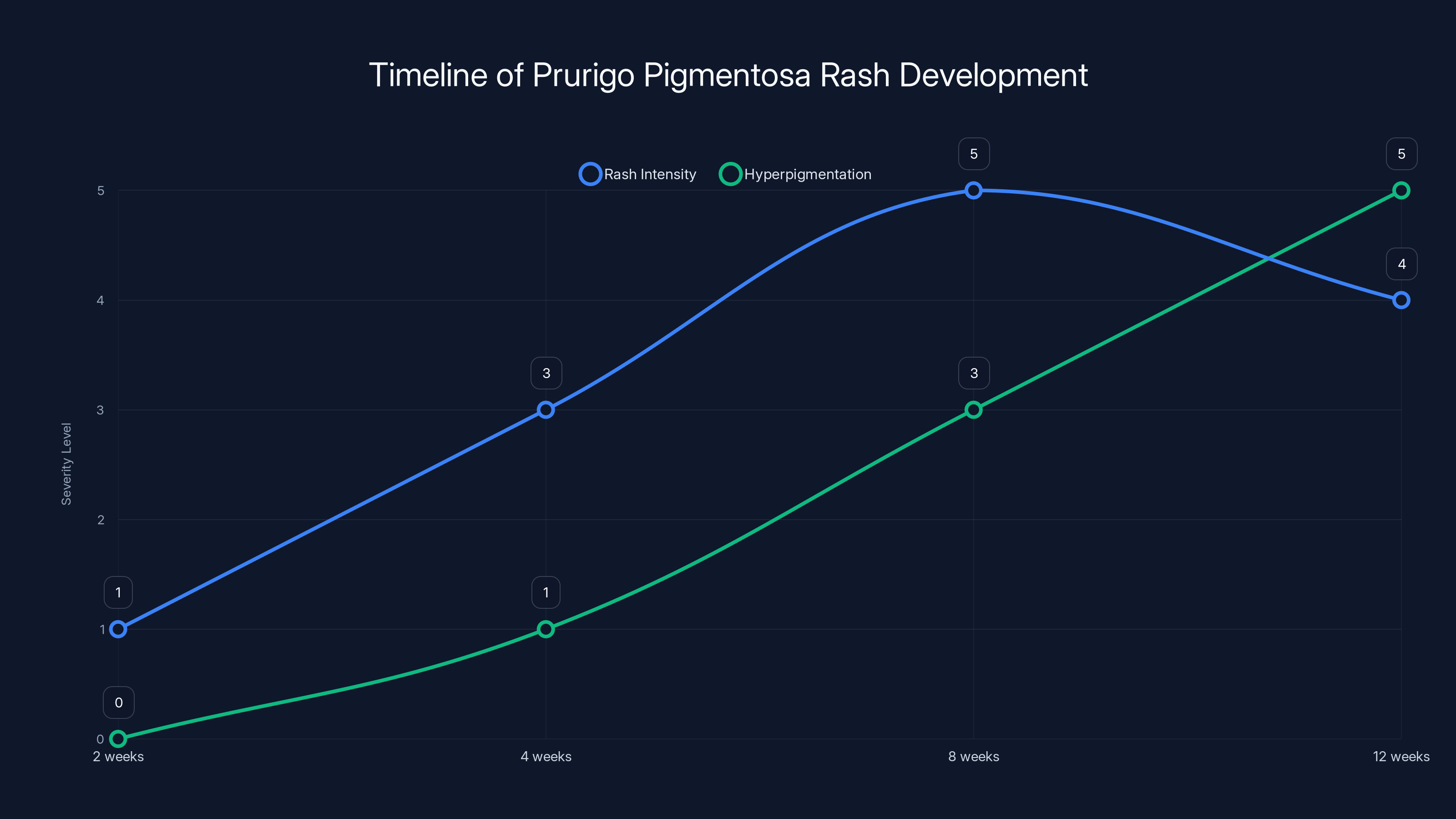
Estimated data shows rash intensity peaking around 8 weeks, with hyperpigmentation increasing over time. Estimated data.
Why Some People Get It and Others Don't: Individual Variation
This is the question that keeps dermatologists up at night. Two people follow identical ketogenic protocols. One develops the rash within weeks; the other follows the diet for years without any skin symptoms. Why?
Genetic factors almost certainly play a role. People with atopic diseases (eczema, asthma, allergies) appear overrepresented in prurigo pigmentosa cases, suggesting a genetic predisposition toward exaggerated inflammatory responses. Family histories of autoimmune or inflammatory conditions may increase risk.
Inflammatory markers might predict susceptibility. Some research suggests elevated baseline inflammatory markers (like C-reactive protein or TNF levels) before starting keto correlate with prurigo pigmentosa risk. If true, this would suggest people with pre-existing inflammatory tendencies are more vulnerable to ketosis-triggered skin inflammation.
Hormonal factors might matter. Women do show higher rates in some studies, though recent data is mixed. Hormonal cycles might modulate immune response. Thyroid function affects metabolism and immune regulation. Cortisol and other stress hormones influence inflammatory pathways.
Microbiome composition probably contributes. Your skin microbiome—the community of bacteria living on your skin surface—changes during ketosis. Different bacterial communities might trigger different immune responses. A person with a protective bacterial community might never develop rashes; another with a more inflammatory community might be susceptible.
Metabolic rate and individual ketone production vary. Two people eating identical meals will achieve different blood ketone levels based on genetics, age, metabolic health, and activity patterns. Perhaps people who produce extremely high ketone levels are at higher risk. Or perhaps the opposite—perhaps efficient ketone utilization is protective, while poor utilization leads to excessive accumulation.
Thermal sensitivity and skin barrier function vary. The rash appears predominantly on areas of potential friction and thermal stress. People with naturally compromised skin barriers or heightened sensitivity might be more susceptible.
Timing of ketone rise might matter. People who shift into ketosis rapidly might trigger a more dramatic immune response than those who transition gradually. This would explain why some people implementing strict keto develop rashes while others adopting lower-carb approaches (which induce ketosis more gradually) escape rashes.
Actual trigger foods might vary. While ketosis itself is the underlying condition, specific foods within the keto diet might amplify inflammation in susceptible individuals. High vegetable oil consumption (promoting omega-6 heavy inflammatory profiles), certain dairy proteins, or mycotoxins in nuts might exacerbate the response.
Physical activity patterns matter. Exercise during ketosis is known to elevate ketone bodies. People engaging in intense training during ketosis might achieve higher ketone levels, potentially increasing rash risk.
The truth is probably multifactorial. Prurigo pigmentosa likely requires convergence of multiple factors: genetic predisposition toward inflammation, a specific metabolic trigger (ketosis), possibly additional dietary or lifestyle factors, and perhaps exposure to conditions (friction, heat) that localize the inflammation to specific body areas.
This complexity explains why the condition is predictable at the population level—we know it's linked to ketosis—yet unpredictable at the individual level. Your specific risk depends on genetics, current health status, and specific implementation details of your ketogenic approach that you might not even be consciously tracking.

The Treatment That Actually Works: Tetracyclines
Here's the remarkable part: once doctors identified the pattern, effective treatments emerged surprisingly quickly. The most studied and most effective treatment is antibiotics from the tetracycline family, specifically doxycycline.
This seems counterintuitive. Prurigo pigmentosa isn't an infection. Cultures are negative. There's no bacterial pathogen. So why do antibiotics work?
Tetracyclines have anti-inflammatory properties independent of their antibiotic effects. They inhibit matrix metalloproteinases, enzymes that break down connective tissue and contribute to inflammation. They suppress cytokine production, damping the inflammatory signal cascade. They inhibit neutrophil recruitment and activation. They even modulate T-cell responses, dampening the adaptive immune system's contribution to inflammation.
These anti-inflammatory effects happen at sub-antimicrobial doses. The doses used for prurigo pigmentosa are often lower than what's needed to treat bacterial infections, yet they prove highly effective.
Doxycycline is the most commonly used tetracycline for prurigo pigmentosa. Typical dosing is 100 milligrams daily for 2-4 weeks. Response is remarkable: most people experience complete or near-complete resolution of symptoms within 7-14 days. The itching stops first. The red lesions fade over days and weeks. The hyperpigmentation gradually resolves over weeks and months.
Other tetracyclines show similar efficacy. Minocycline and tetracycline itself work, though doxycycline is preferred due to better absorption and fewer drug interactions.
But here's the catch: antibiotics are a temporary fix if you continue ketosis. Yes, they resolve the rash. But if you stay in ketosis, the rash often returns after treatment stops. The underlying trigger—ketosis—remains.
That's why the standard recommendation is twofold: take the antibiotic to resolve the acute rash, AND modify diet to exit ketosis. When both happen, the rash typically doesn't recur.
In the Taiwanese man's case, doctors prescribed doxycycline and advised him to stop ketosis. One week later, the rash was gone. He didn't experience recurrence because the metabolic trigger was eliminated.
Alternative anti-inflammatory treatments have been tried with mixed results. Topical steroids provide minimal relief on their own. Systemic corticosteroids work but carry significant side effects for long-term use. Antihistamines are ineffective because histamine isn't the primary driver.
Some emerging evidence suggests certain other medications with anti-inflammatory properties might help. NSAIDs (non-steroidal anti-inflammatory drugs) like ibuprofen provide symptomatic relief and might slow progression, but they're not as effective as tetracyclines.
Recent case reports describe successful use of antimalarial drugs like hydroxychloroquine, which have immunomodulatory properties, but evidence remains limited.
The gold standard remains tetracycline antibiotics combined with dietary modification to exit ketosis.

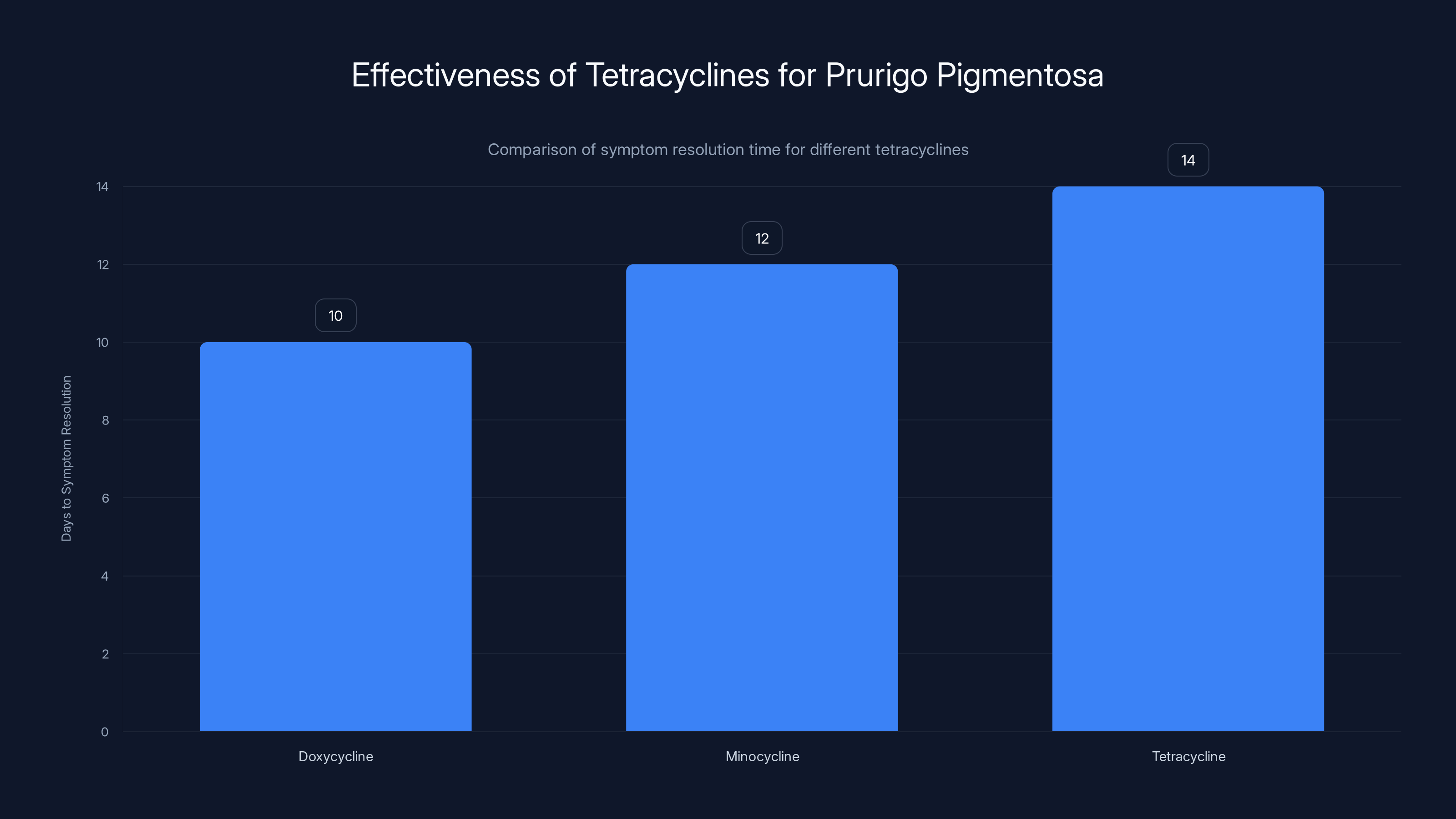
Doxycycline is the most effective tetracycline for prurigo pigmentosa, resolving symptoms in approximately 10 days, followed by minocycline and tetracycline.
Exiting Ketosis: The Direct Solution
The most direct way to resolve prurigo pigmentosa is simply to stop ketosis. Reintroduce carbohydrates. Return to a mixed macronutrient diet. Exit the metabolic state that triggered the inflammatory cascade.
This sounds simple, but it's complicated in practice because most people pursue ketosis intentionally for weight loss or perceived health benefits. Exiting ketosis means abandoning those goals or at least pausing them temporarily.
When people add carbohydrates back, they typically exit ketosis within days. Blood ketone levels drop. The metabolic signal that was triggering immune activation disappears. The inflammatory cascade quiets down.
The rash responds rapidly. Itching usually decreases within 24-48 hours. Visible lesions fade over a week or two. The hyperpigmentation takes longer, sometimes weeks or months, but it typically resolves completely.
The challenge is that some people want to continue ketosis. They've achieved weight loss goals. They feel energized on a ketogenic diet. They're not ready to stop. Is there a way to prevent or manage the rash while maintaining ketosis?
Limited evidence suggests yes, though the approaches aren't universally effective. Some people report that the rash improves spontaneously if they continue ketosis long enough, though this can take months. The inflammatory response might eventually dampen as the body adapts, or the hypothesis goes. But this isn't reliable and means tolerating months of intense itching and visible symptoms.
Other strategies people report as helpful include:
Higher carbohydrate intake within keto: Instead of strict keto (under 50 grams carbs daily), some people shift to a more moderate low-carb approach (100-150 grams carbs daily). This raises blood ketone levels but less dramatically. Some report rash improvement, though they may exit ketosis entirely.
Cyclical keto: Ketogenic during weekdays, higher carb on weekends. The carb refeed days might break the continuous inflammatory stimulus.
Targeted carbs around exercise: Adding carbs perioperationally to workouts might reduce the metabolic stress without eliminating ketosis entirely.
Anti-inflammatory optimization: Maximizing anti-inflammatory foods, omega-3 rich sources, polyphenol-rich vegetables, and minimizing pro-inflammatory seed oils.
Stress reduction and sleep optimization: Both stress and sleep deprivation elevate inflammatory markers. Optimizing these might reduce rash susceptibility.
But none of these are guaranteed. The safest approach remains either accepting that ketosis isn't compatible with your personal inflammatory response and exiting it, or pursuing antibiotics while maintaining ketosis if you're determined to continue.

Prevention Strategies for People Considering Ketosis
If you're considering a ketogenic diet and want to minimize prurigo pigmentosa risk, several strategies might help, though none guarantee prevention.
Start gradually: Rather than jumping into strict keto immediately, phase into lower carbohydrate intake over several weeks. This gradual ketone rise might trigger less immune activation than rapid shifts.
Assess your inflammatory baseline: If you have a history of eczema, psoriasis, or other inflammatory skin conditions, ask your dermatologist about keto compatibility before starting. Your inflammatory predisposition might make you high-risk.
Optimize skin barrier health: Before starting keto, establish a solid skincare routine. Use gentle cleansers, apply moisturizers regularly, and maintain hydration. A robust skin barrier might be more resistant to inflammation.
Anti-inflammatory food optimization: Within ketogenic parameters, emphasize anti-inflammatory foods. Wild-caught fish rich in omega-3s, colorful low-carb vegetables rich in polyphenols, grass-fed meats. Minimize processed seed oils and processed foods.
Monitor for early signs: Know what prurigo pigmentosa looks like. If you notice itchy red bumps on your chest or shoulders within weeks of starting keto, report it to a dermatologist immediately. Early intervention prevents progression.
Have a backup plan: Before starting keto, confirm you have access to a dermatologist and that you'd be willing to take doxycycline or exit ketosis if the rash developed.
Avoid unnecessary triggers: If possible, avoid situations that would amplify any developing rash. Minimize heavy sweating. Avoid tight-fitting clothing that causes friction. Maintain moderate body temperature.
Support your immune system: While this won't prevent rash development if you're predisposed, general immune optimization doesn't hurt. Adequate sleep, stress management, vitamin D sufficiency, and regular moderate exercise all support overall immune function.
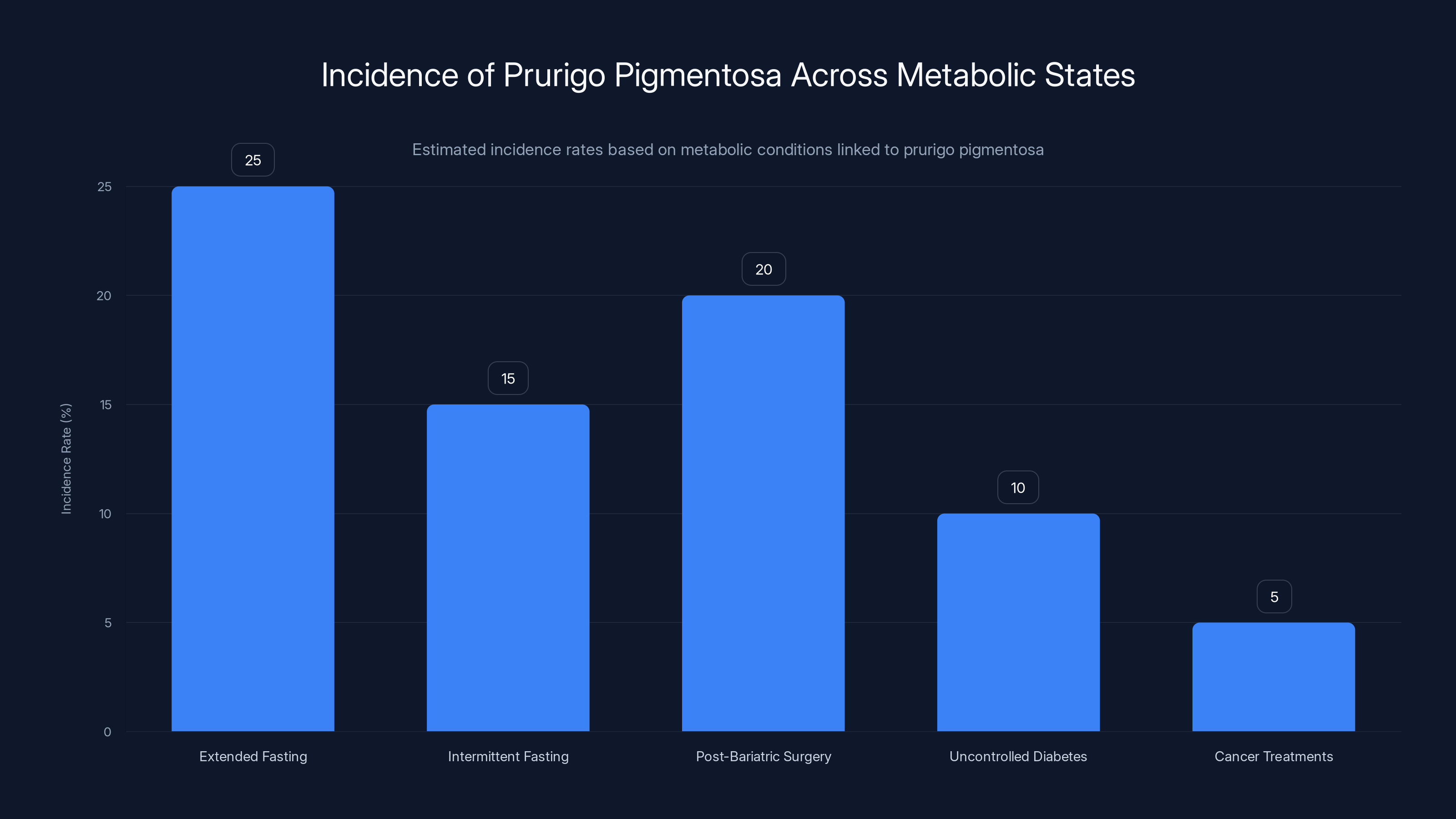
Prurigo pigmentosa appears in various metabolic states, with extended fasting showing the highest estimated incidence rate. Estimated data.
Other Metabolic States Linked to Prurigo Pigmentosa
Ketogenic diets aren't the only condition linked to prurigo pigmentosa. The rash appears across multiple clinical scenarios involving metabolic disruption or sustained ketosis.
Extended fasting: People engaging in longer fasts (24 hours or more) develop ketosis similar to ketogenic diets. Prurigo pigmentosa appears at similar rates in fasting populations as in keto populations.
Intermittent fasting: Particularly extended-window fasts (18-24 hour eating windows), which allow deep ketosis, are associated with prurigo pigmentosa. People doing 16:8 intermittent fasting rarely develop the rash, but those doing OMAD (one meal a day) or longer windows report higher incidence.
Post-bariatric surgery: People who've had weight loss surgery (gastric bypass, sleeve gastrectomy) sometimes develop prurigo pigmentosa even when eating normally. The mechanism isn't purely ketosis-driven; altered nutrient absorption and rapid weight loss appear relevant.
Uncontrolled diabetes: Some people with undiagnosed or poorly controlled type 2 diabetes develop prurigo pigmentosa. The metabolic disruption and lipid metabolism changes might resemble ketosis effects.
Certain cancer treatments: Some chemotherapy agents trigger similar metabolic changes. Cases of prurigo pigmentosa appearing during cancer treatment have been documented.
This diversity of triggers supports the hypothesis that prurigo pigmentosa isn't specific to ketogenic diets but rather represents a skin inflammatory response to sustained ketosis or severe metabolic disruption, regardless of cause.
Long-Term Outlook: Can You Do Keto If You're Prone to the Rash
If you've experienced prurigo pigmentosa during one ketogenic attempt, can you try again?
Yes, but with caveats. The rash doesn't cause permanent skin damage, even though it's incredibly uncomfortable. Once resolved, your skin returns to normal. Hyperpigmentation eventually fades.
But if you're predisposed—if you developed the rash once—you're likely predisposed to develop it again if you return to ketosis. The underlying genetic and inflammatory factors that made you susceptible probably haven't changed.
Some people attempt keto again, get the rash again, take doxycycline again, and manage it. For them, prurigo pigmentosa becomes a manageable side effect of a diet they're committed to. They might ask their dermatologist for a standing prescription for doxycycline, start it immediately if the rash appears, and continue the diet.
Others recognize that ketosis simply isn't compatible with their inflammatory phenotype and choose alternative approaches to weight loss or health optimization. They might do lower-carb diets that don't induce ketosis (50-150 grams daily carbs), intermittent fasting without extreme fasting windows, or other dietary approaches entirely.
The good news is that effective treatment exists. The bad news is that prurigo pigmentosa demonstrates individual variation in how our bodies respond to metabolic states. What works for someone else might not work for you.

The Remaining Mystery: What Researchers Still Don't Know
Despite decades of documented cases and growing medical attention, crucial questions remain unanswered.
Why exactly do ketones trigger neutrophil activation in some people but not others? The immune mechanism appears to involve the inflammasome and pattern recognition receptors, but the specific sensor detecting ketosis remains unknown. Is it direct ketone sensing? Indirect sensing through changes in metabolic byproducts? Sensing of metabolic stress signals?
Why does the rash localize specifically to the chest, shoulders, and upper back? These aren't areas uniquely high in metabolic demand or immune cell concentration. The anatomical specificity suggests local factors—possibly mechanical stress from clothing, thermal stress from environmental exposure, or regional differences in skin barrier function or bacterial colonization.
Why does hyperpigmentation develop alongside and after the inflammation? What triggers melanin overproduction specifically in response to this inflammatory insult?
Are there genetic markers predicting susceptibility? Could genetic testing identify people at risk before starting keto?
Do ketone production rates matter? Do people with extremely high ketone production face higher rash risk, or is absolute blood ketone level what matters?
Could preventive pharmacological interventions exist? Could anti-inflammatory drugs taken preemptively prevent rash development in susceptible people?
These questions matter because answering them could lead to better prediction, better prevention, or better understanding of the underlying mechanisms. They might reveal insights about immune activation relevant to other inflammatory conditions. They might identify modifiable risk factors that could help people with predisposition manage keto more successfully.

Practical Recommendations for Your Ketogenic Journey
If you're considering ketosis or actively following a ketogenic approach, here's what the current evidence suggests:
Know the risk: Prurigo pigmentosa is rare but real. Roughly 1-3 percent of people adopting ketogenic diets develop it. This means 97+ percent don't, but the possibility exists.
Assess your personal risk: Do you have a history of inflammatory skin conditions, atopic diseases, or autoimmune conditions? These might increase your risk. Discuss keto with your dermatologist if you have such history.
Start conservatively: Begin with moderate carb restriction rather than jumping to strict keto. This allows your body to adapt gradually and might reduce rash risk.
Monitor your skin: During the first 3 months on keto, pay attention to your chest and shoulders. Itchy red bumps developing in these specific areas warrant immediate medical evaluation.
Have a plan: Know what prurigo pigmentosa looks like. Know how to access a dermatologist quickly. Know that tetracycline antibiotics are highly effective.
Consider your goals: Be clear about why you're pursuing ketosis. If your goal is rapid weight loss and you're predisposed to the rash, is the trade-off worth it? Could a less restrictive diet achieve your goals without rash risk?
Stay informed: The research on prurigo pigmentosa and ketogenic diets continues. Stay updated on new findings that might affect your approach.
Listen to your body: If the rash develops, that's your body's way of telling you ketosis isn't compatible with your particular physiology. That's not a failure; it's valuable information.

FAQ
What exactly is prurigo pigmentosa?
Prurigo pigmentosa is a specific skin condition characterized by raised, red, itchy bumps typically appearing on the chest, shoulders, and upper back. It's strongly associated with ketosis and metabolic disruption. The condition features inflammation between and around skin cells, with characteristic neutrophil infiltration, and develops in stages, eventually including areas of hyperpigmentation alongside the inflammatory lesions. It's benign but uncomfortable and cosmetically bothersome.
How does ketosis trigger the rash?
Scientists believe elevated ketone bodies trigger an immune response in susceptible individuals, activating neutrophils—a type of white blood cell—which migrate to skin tissue and cause inflammation. The exact mechanism remains unclear, but it likely involves pattern recognition receptors that detect metabolic stress signals associated with ketosis. Ketones themselves appear to be the trigger rather than other aspects of ketogenic diets, since the rash appears across multiple metabolic states producing ketosis (fasting, post-bariatric surgery, certain disease states).
How common is prurigo pigmentosa in people doing keto?
Estimates suggest 1-3 percent of people adopting ketogenic diets develop prurigo pigmentosa, making it relatively uncommon but far from rare in absolute numbers. Given millions of people worldwide following ketogenic diets, thousands likely experience the condition. Rates appear higher in people with pre-existing inflammatory conditions, though more research is needed to identify precise risk factors.
Can you treat the rash while staying in ketosis?
Doxycycline and other tetracycline antibiotics effectively treat the rash through their anti-inflammatory properties, and you can remain in ketosis while taking them. However, the rash frequently recurs once antibiotic treatment ends if ketosis continues. The most reliable approach is combining antibiotics with dietary modification to exit ketosis, which prevents recurrence and allows complete resolution.
How long does the rash take to go away?
With appropriate treatment, the itching typically decreases within 24-48 hours after starting doxycycline or exiting ketosis. Visible inflammatory lesions fade over 7-14 days. Hyperpigmentation takes longer, often several weeks to months, but typically resolves completely. Without treatment while remaining in ketosis, the rash might persist indefinitely, though some people report slow improvement over months.
What should you do if you develop the rash?
Schedule an appointment with a dermatologist immediately. They can confirm diagnosis through examination and, if needed, skin biopsy. Once confirmed, you'll typically be prescribed doxycycline (usually 100 mg daily for 2-4 weeks) and advised to resume carbohydrate intake to exit ketosis. This combination approach provides rapid relief and prevents recurrence. In the meantime, avoid scratching, keep the area clean and dry, and wear soft, non-restrictive clothing to minimize irritation.
Are there ways to prevent the rash if you want to do keto?
While no guaranteed prevention exists, several strategies might reduce risk for susceptible individuals: starting ketosis gradually rather than abruptly, optimizing skin barrier health before beginning, emphasizing anti-inflammatory foods within ketogenic parameters, maintaining stress management and sleep quality, and monitoring closely during the first 3 months for early signs. Most importantly, having a pre-established plan with a dermatologist and being willing to exit ketosis or take antibiotics if the rash develops minimizes complications.
Is the rash dangerous?
No. Prurigo pigmentosa is benign in terms of systemic health. It doesn't threaten organs or cause illness. The discomfort from itching is the primary problem, as is psychological distress from visible symptoms. Scratching can lead to secondary bacterial infection, which is why treatment to stop itching is important. The hyperpigmentation that develops can last months even after inflammation resolves, affecting appearance but not health. Complete recovery is essentially universal with appropriate treatment.
Can the rash leave permanent scars?
Moderate scratching typically causes temporary damage that heals completely. However, intense scratching, particularly if secondary infections develop, can cause atrophic scarring. Preventing this requires stopping the itching cycle, which is why prompt treatment is important. The hyperpigmentation itself isn't scarring but rather melanin overproduction; it fades over time. With appropriate treatment and resisting scratching, permanent scarring is unusual.

Conclusion: Understanding Your Body's Metabolic Signals
Prurigo pigmentosa represents something fascinating about human biology: the diversity of individual responses to identical metabolic states. For most people, ketosis is uneventful, a metabolic tool available for weight management or health optimization. For a small percentage, it triggers a skin inflammatory cascade that's uncomfortable, visible, and psychologically distressing.
This disparity reminds us that biology doesn't operate on universal principles. We inherit genetic susceptibilities. We develop inflammatory phenotypes based on cumulative exposure, infection history, and lifestyle. We exist within ecological communities—our microbiomes—that vary dramatically between individuals. All these factors create a mosaic of individual variation that makes personalized health infinitely more complex than following a one-size-fits-all diet.
The good news is that effective treatments exist. Understanding the mechanism—while incomplete—has led to reliable therapeutic approaches. Doxycycline works. Exiting ketosis works. These aren't mysterious or complicated interventions.
If you're pursuing ketosis for weight loss, metabolic health, or cognitive benefits, the risk of prurigo pigmentosa shouldn't stop you. But it's worth acknowledging, understanding, and monitoring for. If you're predisposed—if you have a history of inflammatory skin conditions or atopic disease—it's worth discussing with a dermatologist before starting.
And if the rash develops despite your intentions and optimism, it's not a failure. It's feedback from your body. Some people can tolerate the rash and manage it with antibiotics while continuing ketosis. Others recognize that ketosis isn't compatible with their physiology and choose alternative paths. Both are legitimate choices based on your priorities, risk tolerance, and circumstances.
The emerging research on prurigo pigmentosa continues to deepen our understanding of immune activation, metabolic signaling, and individual variation in health responses. Each new case report, each clinical trial, adds pieces to the puzzle. Future research will likely reveal the specific immune sensors detecting ketosis, identify genetic markers predicting susceptibility, and perhaps develop preventive strategies for people who want to use ketogenic diets despite inflammatory predisposition.
Until then, we have effective treatments, a growing understanding of who's at risk, and practical strategies for prevention and management. That's not perfect knowledge, but it's real knowledge that improves outcomes. And sometimes that's exactly what medicine can offer: not complete understanding, but enough to help people make informed decisions about their health.
Your body has evolved over hundreds of thousands of years to communicate with you. A sudden, unexplained rash that appears specifically during metabolic shifts is worth listening to. Whether you interpret it as a reason to change course or a manageable trade-off to accept is your decision. But whatever you choose, choose it informed, and choose it in partnership with medical professionals who understand both the cutting-edge research and your individual circumstances.

Key Takeaways
- Prurigo pigmentosa is a documented skin condition specifically linked to ketosis and metabolic disruption, affecting 1-3% of ketogenic dieters
- The rash appears as raised red bumps on the chest and shoulders 3-12 weeks into ketosis, with hyperpigmentation developing over time
- Researchers believe elevated ketone bodies trigger neutrophil-driven inflammation, but the exact mechanism remains incompletely understood
- Doxycycline and other tetracycline antibiotics resolve symptoms within 7-14 days through anti-inflammatory mechanisms unrelated to infection treatment
- Exiting ketosis provides the most reliable permanent resolution, though some people successfully manage the rash while maintaining ketogenic diets
Related Articles
- Boston Dynamics Atlas Robot: The Future of Factory Automation [2025]
- The Madison: Yellowstone Spinoff Release Date, Cast & Everything [2025]
- This Week in Tech: Apple's AI Pin, NexPhone's Triple OS, and the Sony-TCL Merger [2025]
- Microscopic Autonomous Robots Smaller Than Salt: Engineering the Impossible [2025]
- Chelsea vs Arsenal WSL 2025/26: Live Stream, TV Channels & Preview
- 7 Biggest Tech Stories This Week: LG OLED Breakthrough & More [2025]

