![Hypervirulent Klebsiella Pneumoniae: The Bacteria Destroying Eyes [2025]](https://tryrunable.com/blog/hypervirulent-klebsiella-pneumoniae-the-bacteria-destroying-/image-1-1768601258903.png)
Introduction: When A Common Bacteria Becomes A Nightmare
Imagine waking up one morning and losing your vision. Not from age or genetics, but from a bacteria so aggressive it's eating your eye from the inside out. This isn't science fiction. It happened to a 63-year-old man in New England, and his case represents something doctors are watching with growing alarm: the rise of hypervirulent Klebsiella pneumoniae, or hv KP.
For decades, Klebsiella pneumoniae was known as a nuisance. It lingered in hospital corridors, targeting vulnerable patients with weakened immune systems. Doctors knew how to manage it. But hv KP is different. This weaponized version doesn't wait for you to be sick. It doesn't care if you're healthy and strong. It invades healthy people, spreads through the bloodstream like an invading army, and colonizes multiple organs simultaneously.
What makes this story so disturbing isn't just the clinical outcome. It's the mechanism. The bacteria didn't start in the man's eye. It started in his gut after he ate contaminated food. Three weeks later, it had established itself in his liver, lungs, brain, and eye. By the time doctors figured out what was happening, his eye was beyond saving. It had to be surgically removed.
This case, published in a recent issue of the New England Journal of Medicine, tells us something critical: hv KP is spreading globally, and we're only beginning to understand how dangerous it truly is. Between 2020 and 2024, reported cases of hv KP infections in the United States increased significantly. International surveillance data suggests the bacterium is now circulating in at least 18 countries across four continents.
What's particularly terrifying is how hv KP behaves differently than its classical cousin. While normal Klebsiella pneumoniae causes localized infections, hv KP causes metastatic disease. It doesn't settle in one place. It travels. It invades. It destroys multiple organ systems before a diagnosis is even made.
For this reason, understanding hv KP matters. Whether you're a healthcare provider, a patient, or someone simply concerned about emerging infectious diseases, knowing how hv KP works, how it spreads, and what to watch for could save your life or the life of someone you care about.
Let's break down everything you need to know about this bacterium, from its origins to its devastating consequences to the latest diagnostic and treatment advances.
TL; DR
- Hypervirulent Klebsiella pneumoniae (hv KP) is an aggressive bacteria that infects healthy people, not just hospital patients
- Metastatic spread means hv KP travels throughout the body, attacking the liver, lungs, brain, eyes, and soft tissues simultaneously
- One patient's case shows how hv KP can destroy an eye completely (panophthalmitis), require surgical removal, and infiltrate the brain
- Diagnosis is difficult because traditional tests can't easily distinguish hv KP from classical K. pneumoniae without genetic testing
- Early recognition and aggressive antibiotics offer the best chance of survival, but organ damage may already be irreversible
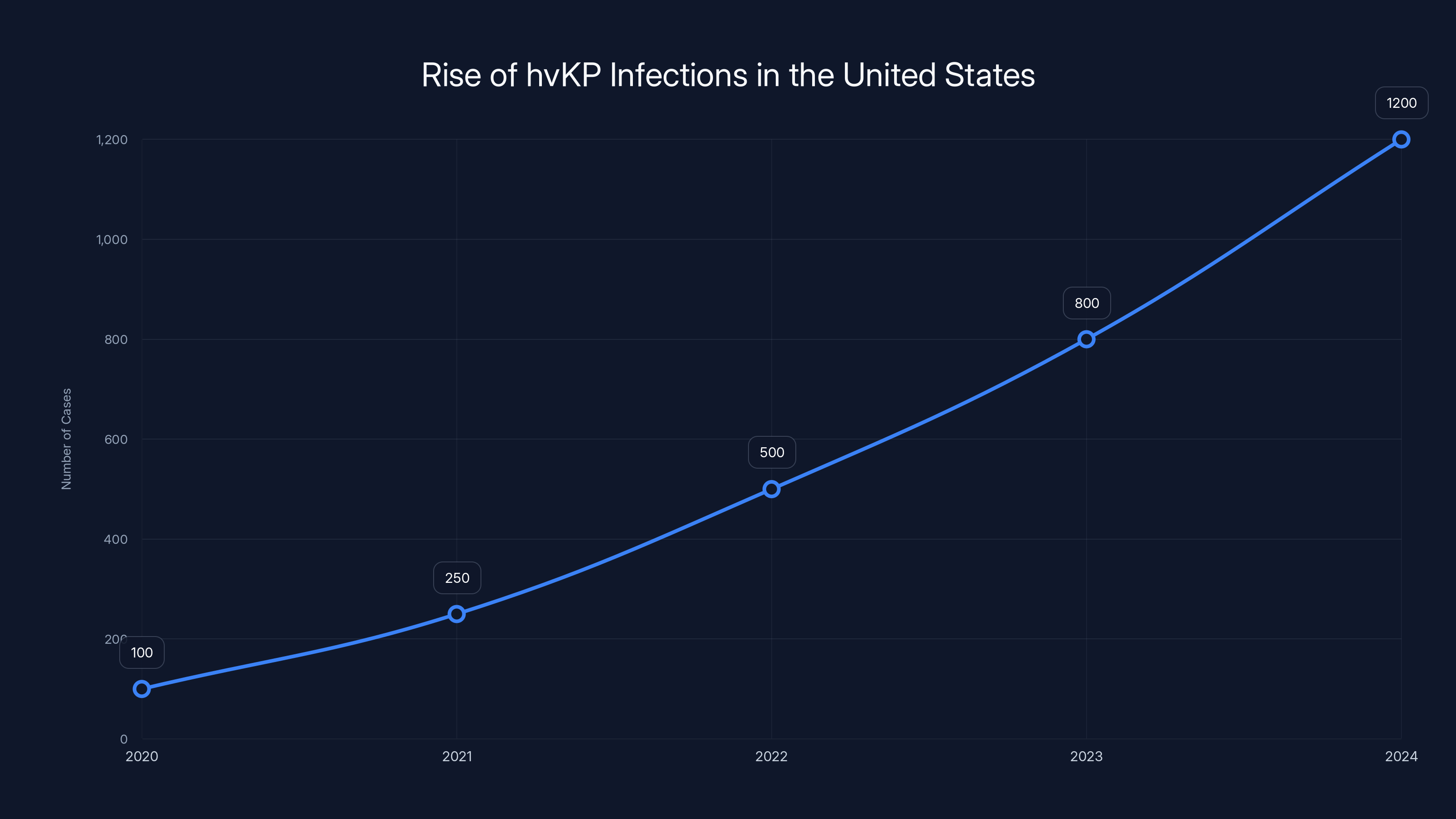
Reported cases of hypervirulent Klebsiella pneumoniae (hvKP) in the United States have shown a significant upward trend from 2020 to 2024. Estimated data.
The Classical Klebsiella: Understanding The Baseline
Before we can understand what makes hv KP so dangerous, we need to understand its predecessor. Klebsiella pneumoniae isn't inherently evil. In fact, it's a normal inhabitant of the human gut. Most people carry it without any problems whatsoever.
Classical K. pneumoniae became famous in hospital settings. For the past 40 years, it's been one of the leading causes of hospital-acquired infections. It causes pneumonia in patients on ventilators. It causes urinary tract infections in people with catheters. It causes bloodstream infections in immunocompromised individuals. Nurses and infection control specialists know this bacterium well.
The key characteristic of classical K. pneumoniae is its opportunistic nature. It's a predator that hunts the weak. It waits for compromised immunity, for disrupted barriers, for vulnerable patients. In a healthy person with a functioning immune system, classical K. pneumoniae rarely causes serious disease. Your body's defenses contain it. Your white blood cells neutralize it. Your immune system keeps it in check.
This predictability made classical K. pneumoniae manageable. Doctors understood the risk factors. They knew which patients needed special attention. They implemented protocols to prevent spread. The bacterium followed the rules of opportunistic infection.
Then something changed. In the 1980s, researchers in Taiwan started noticing something strange. Young, previously healthy people were showing up with severe liver infections. No prior surgery. No compromised immunity. No obvious risk factors. Yet they had massive, life-threatening abscesses in their liver. Further investigation revealed that a variant of K. pneumoniae was responsible, and it wasn't behaving like the classical version.
This variant had acquired genetic material that made it fundamentally different. It was more aggressive. It was more invasive. It produced more virulence factors. It could establish systemic infections in people whose immune systems were working perfectly fine. Over the following decades, this hypervirulent strain spread from Asia to North America, Europe, and beyond.
By 2020, hv KP had become a global concern. Case reports began appearing in medical literature with increasing frequency. Patients presented with unusual presentations: liver abscesses in young, healthy people. Meningitis in otherwise well individuals. Eye infections in people who'd never had eye surgery. The pattern was clear: this wasn't your grandmother's Klebsiella pneumoniae.

The New England Case: A Clinical Thriller
Our story begins with a 63-year-old man in the New England region who did something most of us have done: he ate something that disagreed with him. According to his account, he consumed what he believed to be spoiled meat. Within hours, the consequences were evident. He developed severe vomiting and diarrhea. His gastrointestinal system was actively rejecting whatever pathogen the contaminated food contained.
Here's where the timeline becomes critical. These initial gastrointestinal symptoms lasted about two weeks. The man experienced the typical course of foodborne illness: misery followed by recovery. He got better. His vomiting stopped. His diarrhea resolved. By all accounts, he seemed to have weathered the storm.
But he hadn't. The bacteria had other plans.
Three weeks after his initial illness, new symptoms emerged. This time, it wasn't his gut that was the problem. He developed a persistent cough. Chills set in. A fever climbed. He felt progressively worse, and unlike his initial episode, these symptoms didn't improve with time. They intensified. His cough became relentless. The fever spiked higher. The chills became severe enough that they disrupted his sleep.
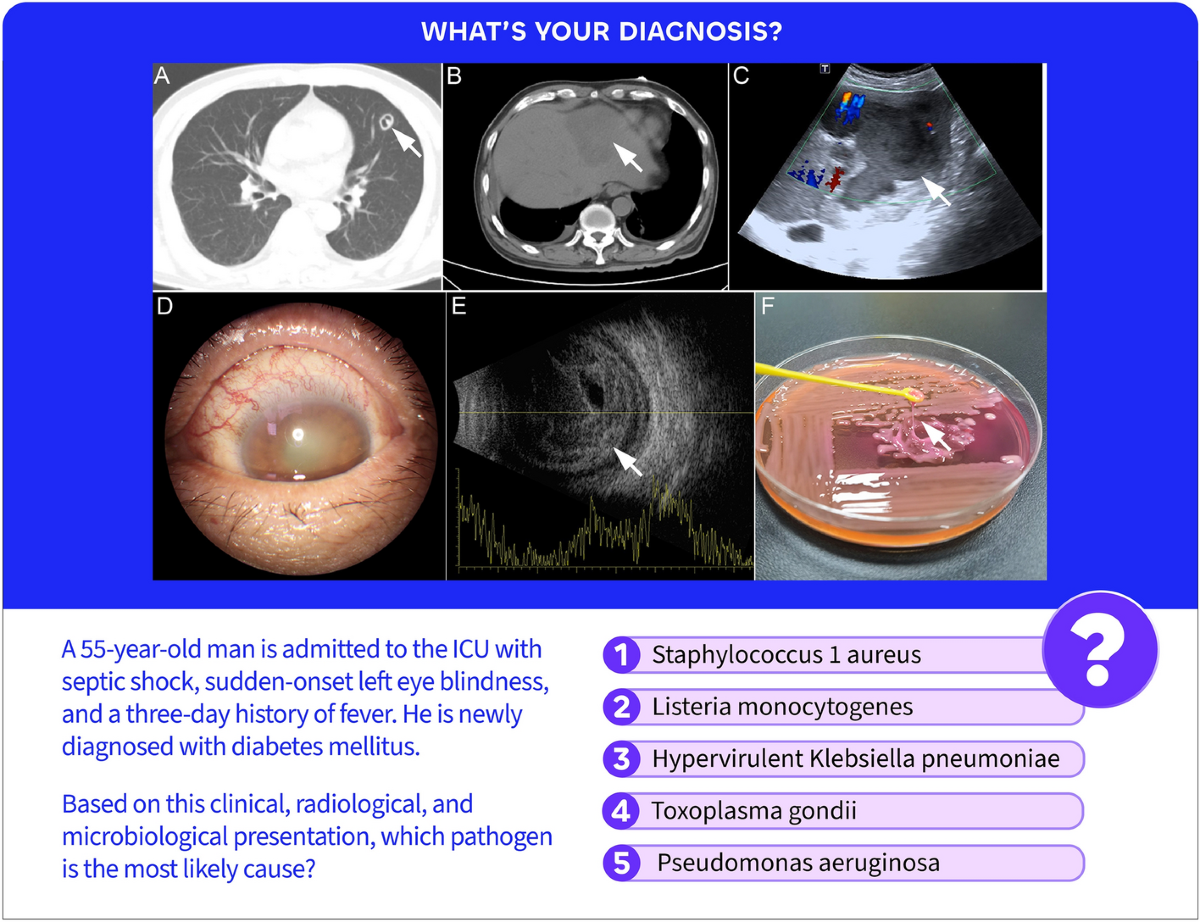
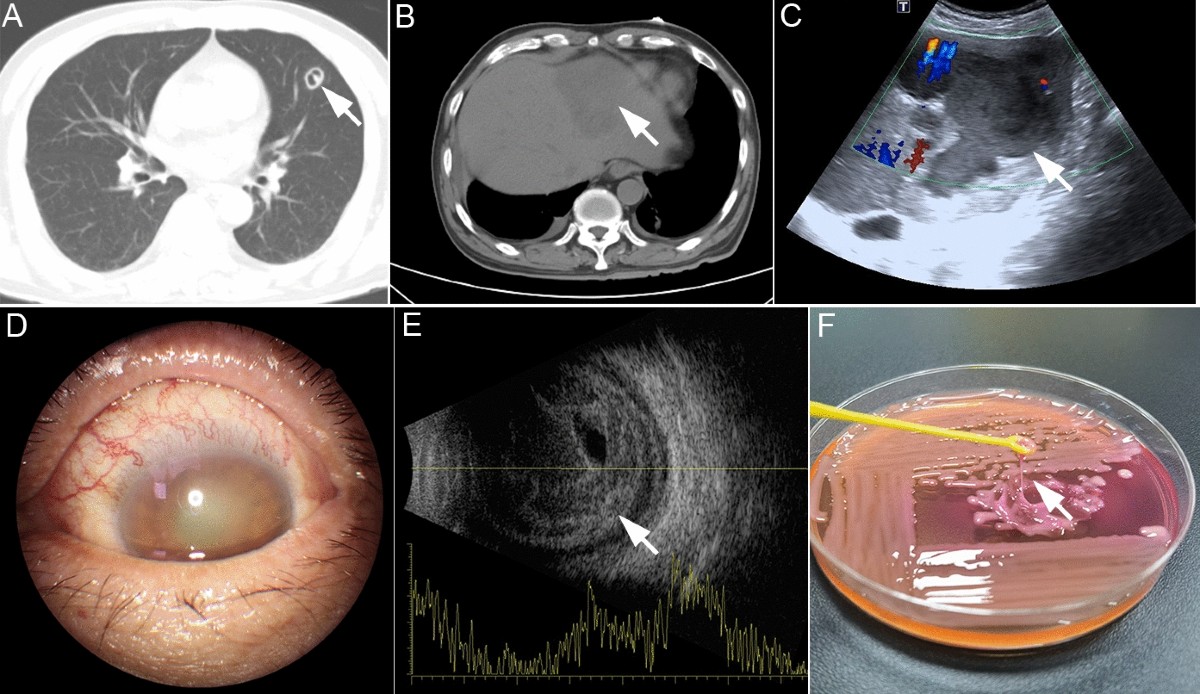
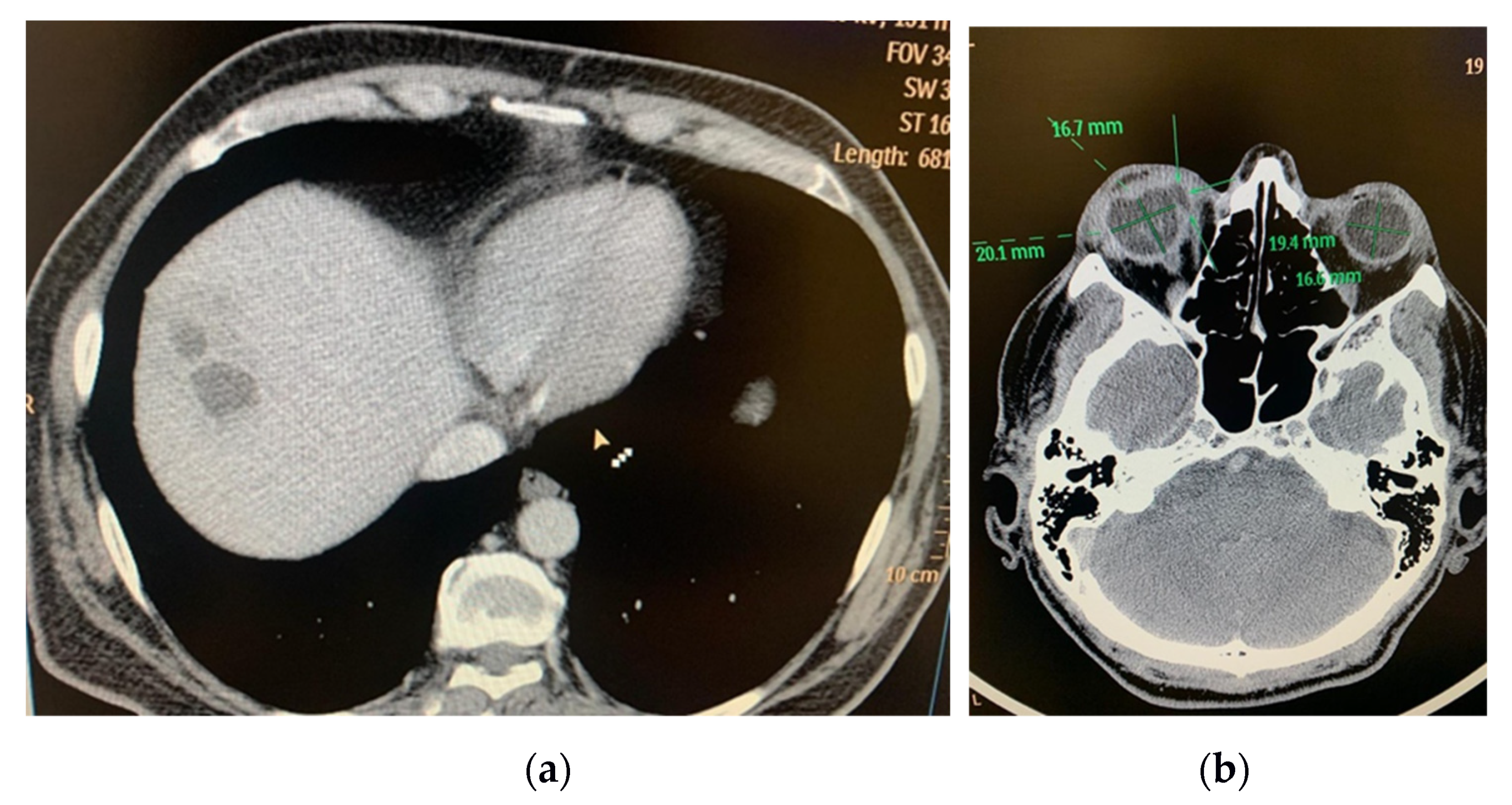
After suffering through several days of worsening respiratory symptoms, he made the decision to go to the hospital. This is where modern medicine's diagnostic capability enters the story. The emergency department team obtained imaging studies: X-rays and CT scans of his chest and abdomen. The images revealed something alarming: over 15 distinct nodules and masses scattered throughout both lungs.
But the lungs weren't the only problem. The imaging also showed a large mass in his liver measuring 8.6 centimeters in diameter, roughly the size of a golf ball. For context, a normal liver is smooth and homogeneous. Masses like this suggest infection, inflammation, or malignancy. The clinical picture was becoming more ominous.
Laboratory work supported an infectious process. Doctors started him on supplemental oxygen for his respiratory compromise and broad-spectrum antibiotics while they worked to identify the specific culprit. He was admitted to the hospital for monitoring and treatment.
For the first two days, he received appropriate supportive care. His oxygen saturation improved. He was on antibiotics. The medical team was working the case systematically. But on his third hospital day, something new occurred. He woke up unable to open his right eye. His vision in that eye was gone. The eyelid was swollen to the point where he physically couldn't pry it open.
An MRI was ordered to evaluate this new development. The results added another layer to the clinical puzzle: his brain contained multiple lesions. These weren't small, subtle findings. Multiple areas of his brain showed evidence of infection or inflammation. The case had just jumped from a patient with disseminated infection of his lungs and liver to a patient with metastatic disease involving three separate organ systems: lungs, liver, and brain.
He was transferred to Massachusetts General Hospital for higher-level care. At this point, the clinical team was dealing with a genuinely rare and severe presentation. The key to solving the puzzle, as it would turn out, was the eye.

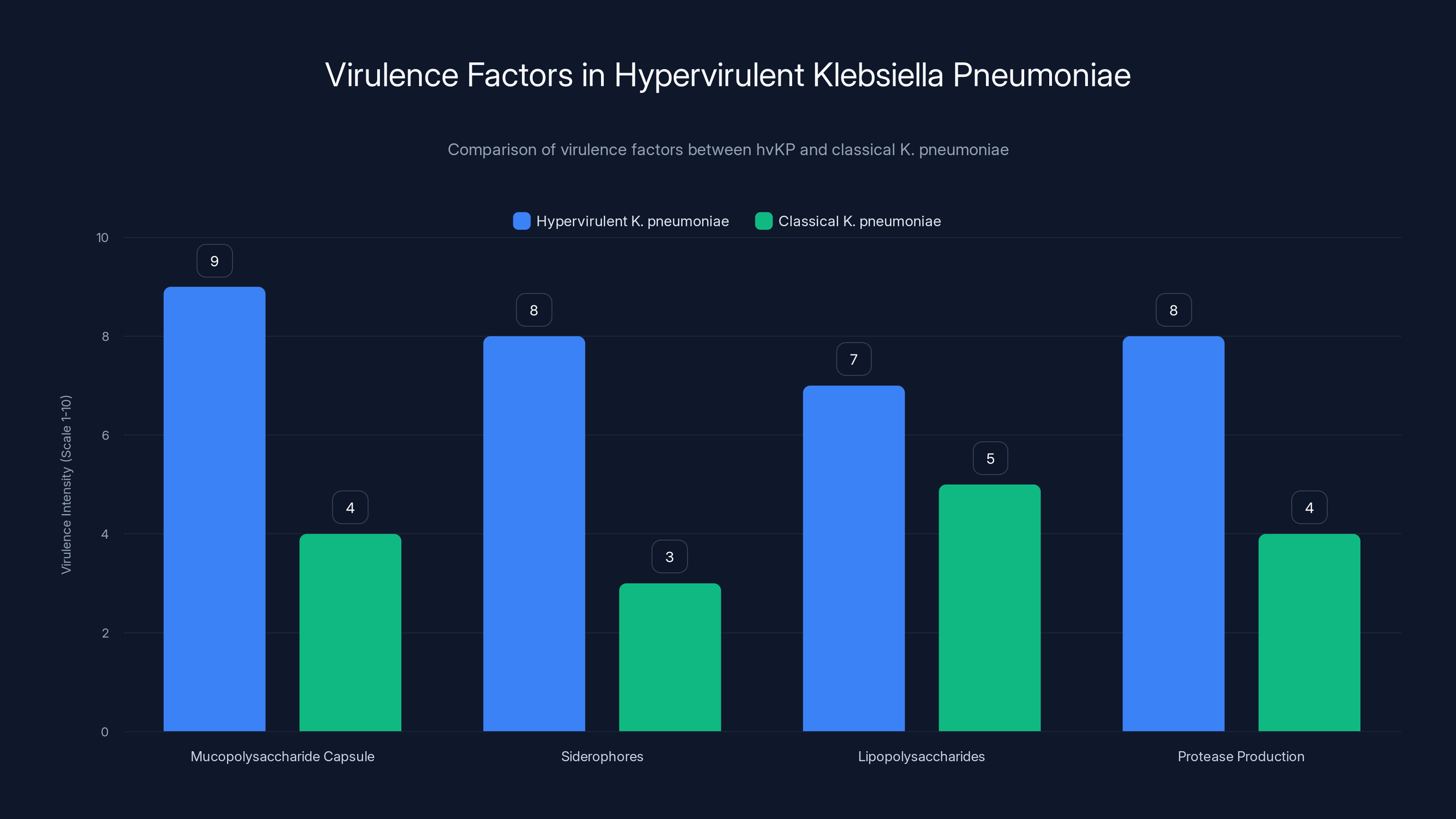
Hypervirulent K. pneumoniae exhibits significantly higher levels of virulence factors compared to classical strains, particularly in capsule thickness and siderophore production. Estimated data based on qualitative descriptions.
Panophthalmitis: When The Eye Becomes A Battlefield
When the man's eye began swelling, ophthalmologists were consulted. What they found was not a simple eye infection. The condition is called endophthalmitis, which means infection of the internal structures of the eye, specifically the vitreous humor and aqueous humor (the gel and liquid portions inside the eye).
Endophthalmitis is rare but serious. In most cases, it results from a clear mechanism: an eye injury that allows bacteria to enter, or a recent eye surgery that introduced infection. The man had neither. His eye had never been injured. He'd never had ocular surgery. Yet he had a raging internal eye infection.
But even more concerning was the severity. His condition wasn't limited to infection of the internal fluids. His eye showed signs of panophthalmitis, which means all layers of the eye are infected and inflamed. This is extraordinarily rare and extraordinarily devastating. The eyelid is swollen. The sclera (white of the eye) is inflamed. The muscles that move the eye are swollen. The orbital tissue surrounding the eye is inflamed. Every anatomical structure is involved in the infectious process.
Panophthalmitis is not something a patient recovers from with vision intact. This is a condition that ends in blindness or surgical removal of the eye. There's no middle ground. The inflammation and infection cause irreversible damage to the structures responsible for vision, particularly the retina and optic nerve.
Clinically, the question became: how did this infection start? The standard mechanism for endophthalmitis didn't apply. This man's infection didn't come from external trauma. It came from inside. The bacteria must have been circulating in his bloodstream and lodged in his eye, establishing infection from the inside out. This is called endogenous endophthalmitis, and it's far less common than externally-acquired cases.
Endogenous endophthalmitis typically occurs in patients with serious bloodstream infections. The bacteria are circulating in sufficient quantities and with sufficient virulence that they seed distant sites including the eye. In immunocompromised patients, this can happen with relatively low-grade infections. But in immunocompetent individuals, it requires an unusually aggressive pathogen.
The clinical team realized they were dealing with something systematically unusual. A bacterium that:
- Started as a gastrointestinal infection after contaminated food
- Spread to establish a large liver abscess
- Colonized multiple areas of both lungs
- Invaded the brain and established multiple lesions
- Circulated in sufficient numbers to seed and establish infection in all layers of the eye
This pattern of widespread, metastatic infection in a previously healthy person pointed to one specific diagnosis: hypervirulent Klebsiella pneumoniae.
Hypervirulent Klebsiella Pneumoniae: The Weaponized Variant
Hypervirulent Klebsiella pneumoniae is a fundamentally different organism from its classical predecessor. The differences aren't just in degree but in kind. Think of it this way: classical K. pneumoniae is an opportunistic street criminal that preys on the weak. hv KP is a trained soldier that can assault the strongest fortifications.
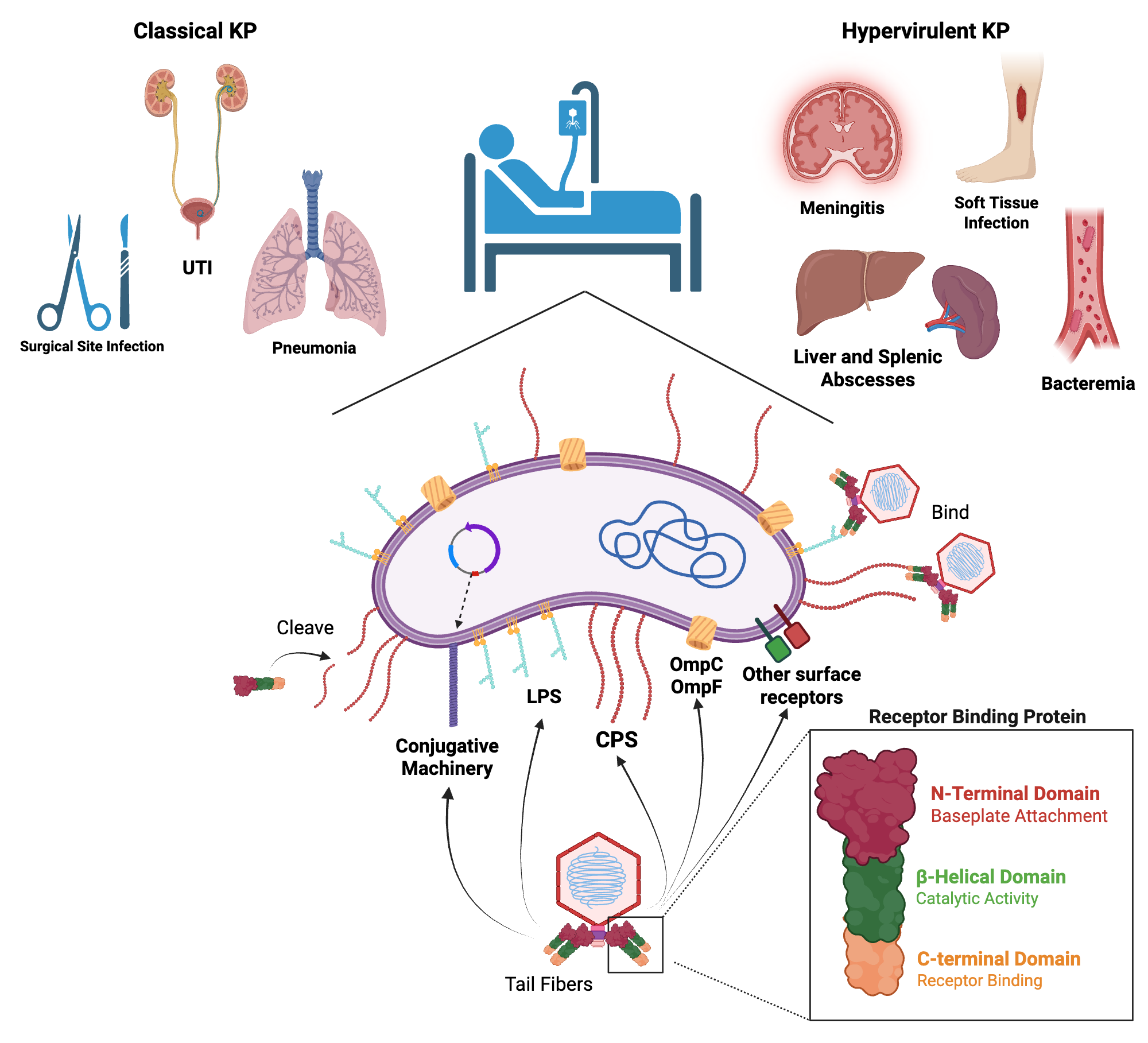
The bacterial cell is the same basic organism, but it carries additional genetic material that dramatically alters its behavior. This genetic material comes in the form of plasmids, which are circular pieces of DNA separate from the chromosome. Plasmids can replicate independently and be shared between bacteria through a process called conjugation. hv KP strains carry plasmids that encode for enhanced virulence factors.
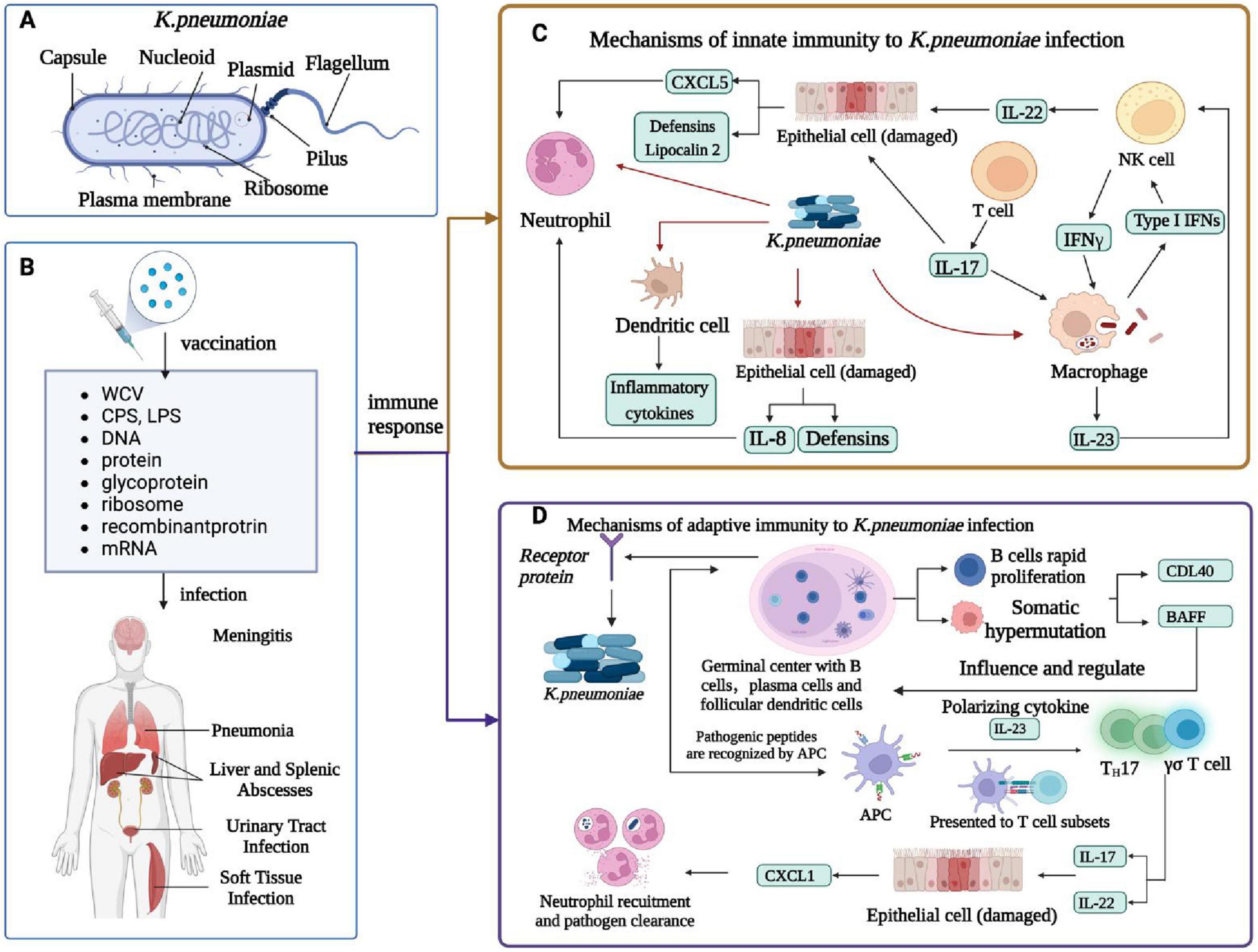
These virulence factors include:
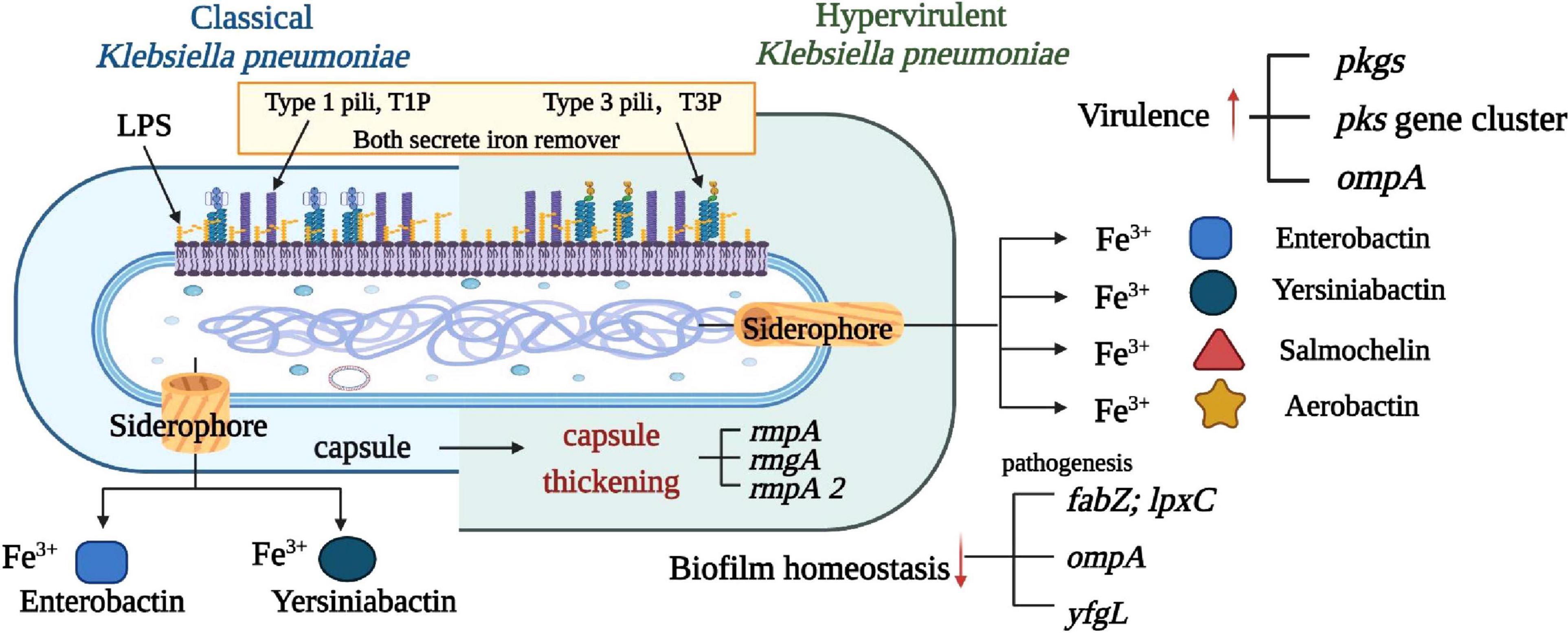
Mucopolysaccharide capsule: hv KP produces an exceptionally thick, mucoid capsule around its cell wall. This capsule makes the bacterium incredibly sticky and also helps it evade the immune system. The capsule is so pronounced that it gives hv KP colonies a distinctive appearance on culture plates—they're gelatinous and viscous compared to the drier colonies of classical K. pneumoniae.
Siderophores: These are molecular iron-scavenging compounds. Iron is essential for bacterial growth, but in the human body, iron is sequestered by proteins like transferrin and lactoferrin. hv KP produces multiple siderophore systems that are exceptionally efficient at extracting iron from these host proteins, giving hv KP a significant metabolic advantage in human tissues.
Lipopolysaccharides and other surface antigens: hv KP's cell surface contains different lipopolysaccharide (LPS) configurations that are more immunogenic and more resistant to complement-mediated killing compared to classical strains.
Protease production: hv KP produces more and more aggressive proteases that break down host proteins, allowing the bacterium to spread through tissue barriers more efficiently.
The cumulative effect of these factors is transformative. hv KP doesn't simply infect a patient. It aggressively invades, spreads, and establishes itself in multiple organ systems simultaneously. The bacterial load in infected patients tends to be higher. The inflammatory response is more severe. The tissue damage is more extensive.
One of the hallmark features of hv KP infection is liver abscess formation. Classical K. pneumoniae causes liver infections, but typically in hospitalized patients or those with risk factors like biliary obstruction or cirrhosis. hv KP causes massive liver abscesses in young, healthy people with no risk factors. The first reports came from Taiwan in the 1980s and 1990s, where clusters of healthy young people presented with overwhelming liver infections caused by this strain.
The geographic origin likely relates to food and water contamination patterns in East Asia, but hv KP has since spread globally. The mechanism of spread appears to involve multiple routes: contaminated food sources, water supplies, and possibly person-to-person transmission in certain settings.
The Metastatic Nature Of hv KP Infection
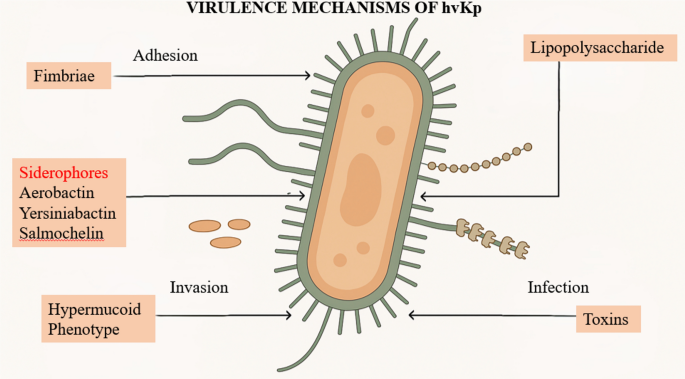
What distinguishes hv KP infections from classical K. pneumoniae is the pattern of dissemination. Classical K. pneumoniae typically causes focal infections: a pneumonia, a urinary tract infection, a bloodstream infection centered on a specific source. hv KP, by contrast, causes metastatic disease. Once it enters the bloodstream, it spreads throughout the body and establishes satellite infections in multiple organ systems.
The typical progression of hv KP infection follows a recognizable pattern. It usually begins with a gastrointestinal source, often food-borne. The bacterium penetrates the intestinal barrier and enters the bloodstream. Once bacteremia is established, the organism shows a particular tropism for the liver. In the liver, hv KP establishes large, pus-filled abscesses. These aren't small, localized infections. They're often multiple, sometimes with aggregate diameters exceeding 10 centimeters.
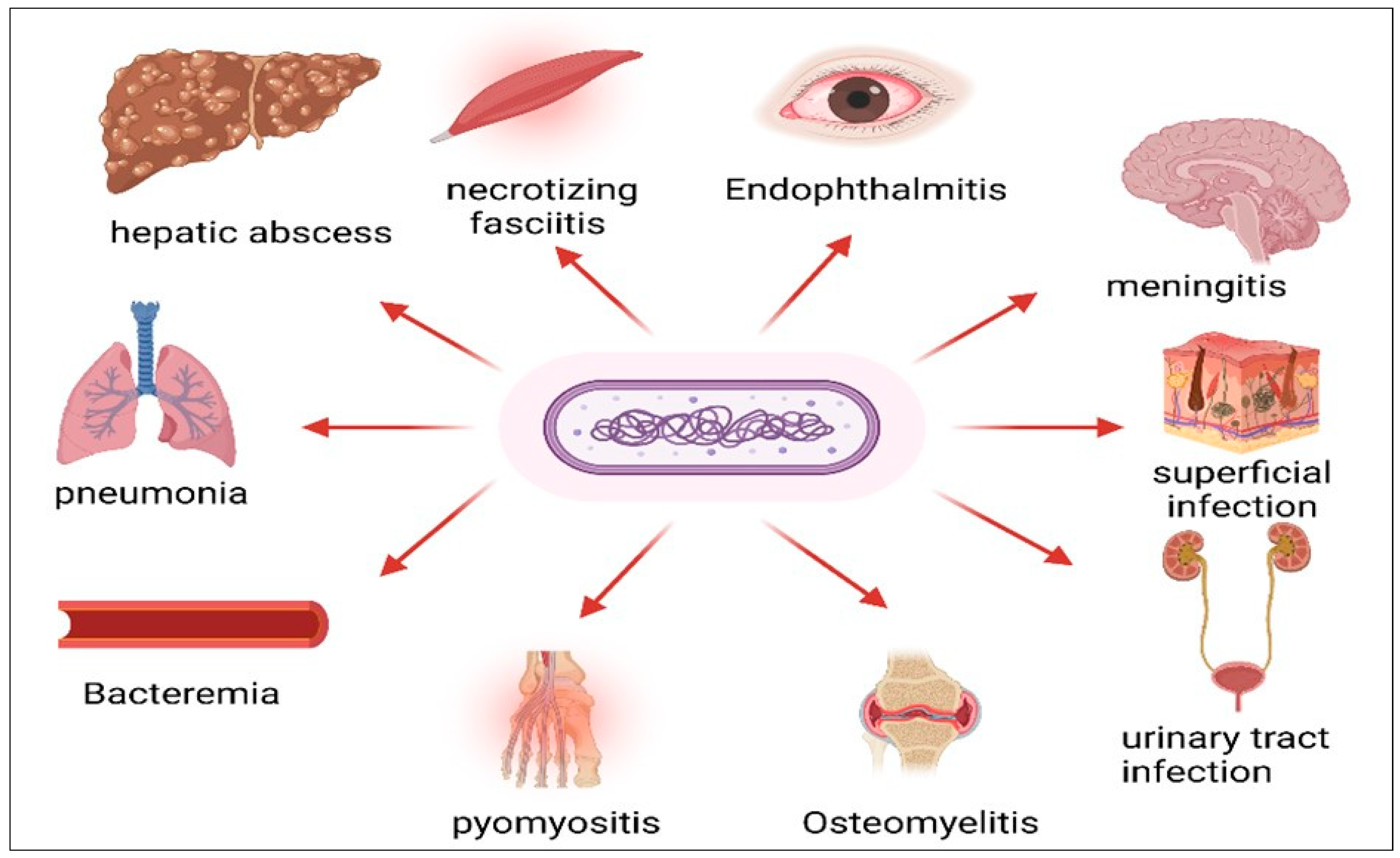
From the liver, the bacteria disseminate further. Through the bloodstream, hv KP spreads to the lungs, causing pneumonia and nodular infiltrates. It reaches the central nervous system, causing meningitis or brain abscesses. It seeds the soft tissues, establishing cutaneous infections. And in some cases, it reaches the eye through blood vessels supplying the orbital and ocular tissues.
The reason hv KP prefers the liver likely relates to the unique environment of hepatic tissue. The liver is highly vascularized, providing excellent access for circulating bacteria. The liver also has a large population of immune cells (Kupffer cells), but in hv KP infection, the virulence factors appear sufficient to overwhelm these defenses. Once established in the liver, the abscess becomes a reservoir of bacteria that continuously seed other sites through the bloodstream.
This metastatic pattern explains why hv KP infections are so dangerous. Even if you treat the primary source—even if you successfully clear the bacteria from the lungs or other infected tissues—if the liver abscess isn't adequately drained and treated, the infection will recur. The bacteria will continue to circulate and establish new infections in distant organs.
In the New England case, the man's infection followed this classic pattern. The initial gastrointestinal exposure led to bacteremia. The bacteria lodged in his liver, creating the large 8.6 cm abscess. From there, the infection spread to his lungs (multiple nodules), his brain (multiple lesions), and his eye (panophthalmitis). This progression is textbook hv KP.
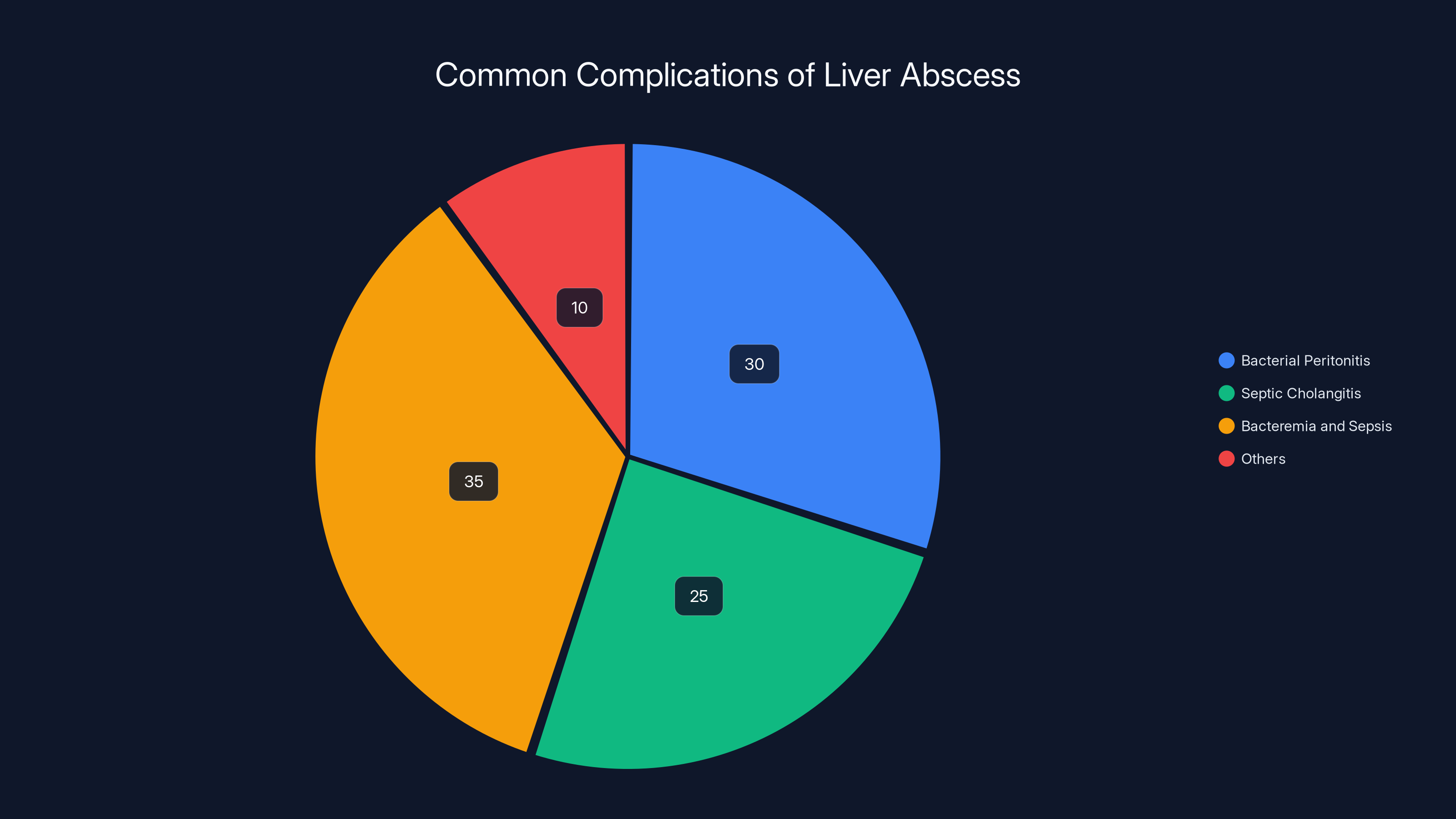
Estimated data shows that bacteremia and sepsis are the most common complications of liver abscesses, followed by bacterial peritonitis and septic cholangitis.
Diagnosis: The Challenge Of Distinguishing Hypervirulent From Classical
Here's where the story gets particularly challenging for clinicians: you can't easily tell the difference between hypervirulent and classical Klebsiella pneumoniae just by looking at it. They're the same species. They grow on the same culture media. Standard bacterial identification systems may classify them identically.
In the New England patient's case, respiratory cultures grew Klebsiella pneumoniae. The lab identified it as K. pneumoniae. But that identification doesn't specify hypervirulent status. Without additional testing, the clinical team wouldn't know whether they were dealing with a classical strain or a hypervirulent one.
For years, this was a major diagnostic gap. Doctors would treat K. pneumoniae infections empirically with antibiotics effective against the species as a whole. But not knowing the virulence status of the strain left clinicians flying blind when it came to predicting disease severity and progression.
In recent years, researchers have developed methods to identify hv KP more specifically. The most scientifically rigorous approach involves genetic sequencing and identification of specific virulence genes. hv KP strains characteristically carry five virulence-associated genes on plasmids: aerobactin synthesis (iuc A), salmochelin synthesis (iro A), allantoin metabolism (all A), propanediol utilization (pdu A), and transcriptional regulator (rmp A). The presence of these genes, particularly multiple genes in combination, is highly suggestive of hv KP.
However, genomic sequencing isn't practical as a rapid diagnostic test in most clinical settings. It takes time, it's expensive, and not all hospitals have the capability. Doctors need something faster.
This is where the string test comes in. The string test is simple, low-cost, and can be performed in any microbiology laboratory. Here's how it works: you grow the suspected K. pneumoniae on a blood agar plate or another standard medium. You take an inoculation loop and touch it to a colony of the bacterium, then lift the loop away from the plate. If the colony has an unusually mucoid, sticky consistency, a string of bacterial goo will stretch upward from the plate. If the string extends more than 5 millimeters before breaking, the test is considered positive for hv KP.
Is the string test perfect? No. It's a surrogate marker, not a definitive identification. Some classical K. pneumoniae strains may produce sufficient mucoid material to yield a positive string test. Conversely, some hv KP strains might produce a less robust mucoid phenotype and score negative. But in clinical practice, a positive string test in a patient with the appropriate clinical presentation (metastatic infection, liver abscess, brain lesions, endophthalmitis) is highly suggestive of hv KP.
In the New England case, the string test on the respiratory isolate was positive, supporting the hv KP diagnosis. This relatively simple test ended up being the key to the diagnostic puzzle.

The Five Virulence Genes: Molecular Basis Of Hypervirulence
Understanding why hv KP is so dangerous requires diving into the molecular basis of its virulence. The genetic elements that separate hv KP from classical K. pneumoniae are well-characterized, though the research continues to evolve.
The five genes most commonly associated with hv KP are found on plasmids and encode for specific metabolic and immunological advantages:
Aerobactin synthesis (iuc A and related genes): Aerobactin is a powerful siderophore that hv KP produces to sequester iron from the host environment. Iron is essential for bacterial growth, and in the human body, free iron is essentially nonexistent. All iron is bound to proteins. hv KP's aerobactin system is particularly efficient at extracting iron from transferrin and lactoferrin, the primary iron-transporting proteins in blood and body fluids. This gives hv KP a significant metabolic advantage, allowing faster growth and higher bacterial loads in infected tissues.
Salmochelin synthesis (iro A and related genes): This is another siderophore system, complementing the aerobactin pathway. Having multiple iron-acquisition systems provides redundancy and ensures that hv KP can access iron even if the host upregulates one defense mechanism.
Allantoin metabolism (all A and related genes): This gene cluster allows hv KP to metabolize allantoin, a breakdown product of purine metabolism found in infected tissues. This provides hv KP with an alternative nutrient source that classical K. pneumoniae cannot access efficiently. In the context of a localized infection, this might seem minor. But in the context of a large, walled-off liver abscess, the ability to utilize alternative nutrient sources could mean the difference between an abscess that shrinks and one that persists or enlarges.
Propanediol utilization (pdu A and related genes): Similarly, this gene cluster allows hv KP to metabolize propanediol, another organic compound present in infected tissues. Again, this provides hv KP with metabolic flexibility that classical strains lack.
Transcriptional regulator (rmp A and related genes): This gene encodes for a regulator that controls the expression of mucoid phenotype genes. hv KP strains with functional rmp A genes typically produce higher amounts of capsular polysaccharides, creating the characteristic mucoid appearance and enhanced immune evasion.
The presence of these genes, particularly when multiple genes are detected simultaneously, defines the hv KP phenotype at the genetic level. A classical K. pneumoniae strain might have one or even two of these genes but typically not all five.
What's particularly important is that these genes are carried on plasmids, which means they can theoretically be transferred between bacteria. In theory, a classical K. pneumoniae strain could acquire these plasmids from an hv KP strain and become hypervirulent itself. This is a source of concern for epidemiologists monitoring the spread of hv KP. The genetic elements of hypervirulence aren't locked into the chromosome. They're mobile.
Organ Tropism: Why The Liver First?
One of the most consistent features of hv KP infection is its tropism for the liver. The overwhelming majority of hv KP cases involve hepatic abscess formation. Some cases involve other organs, but the liver is almost always on the list of affected sites. Why is the liver such a favored target for hv KP?
Several factors likely contribute:
Vascular anatomy: The liver receives blood from two sources: the hepatic artery and the portal vein. The portal vein carries nutrient-rich blood from the gastrointestinal tract. If hv KP enters the bloodstream through the GI tract (which is the typical route), it reaches the liver via the portal circulation. The liver is essentially the first major organ that circulating bacteria encounter.
Hepatic blood flow and filtration: Despite receiving a large blood flow, the liver is not an efficient filter for bacteria compared to the spleen. While the spleen is rich in macrophages that aggressively phagocytose circulating bacteria, the liver's Kupffer cells (resident macrophages) are somewhat less aggressive. This allows bacteria to establish themselves in the liver more easily than in some other organs.
Nutritional environment: The liver is an extraordinarily metabolically active organ. It contains abundant nutrients, including amino acids, carbohydrates, and other organic compounds. For a growing bacterium, the liver is a feast. Additionally, the liver's role in iron metabolism means there are mechanisms for iron sequestration and availability that hv KP's virulence factors have evolved to exploit.
Bile composition: The liver produces bile, which contains antimicrobial compounds. However, bile also contains nutrients and has a p H and osmolarity that favors bacterial growth in certain niches. The balance between antimicrobial and permissive factors may favor hv KP more than classical strains.
Immunological factors: The liver has unique immunological properties. While it contains immune cells, it also has mechanisms that promote tolerance. The liver is exposed to constant bacterial antigens from the GI tract, and it has evolved to be relatively tolerant of low-level bacterial exposure. hv KP's virulence factors may exploit this tolerance.
Once an hv KP abscess becomes established in the liver, it becomes a chronic source of bacteria that continuously seed other organs. Patients with hv KP infection and liver abscess are at high risk for disseminated disease unless the abscess is aggressively treated.

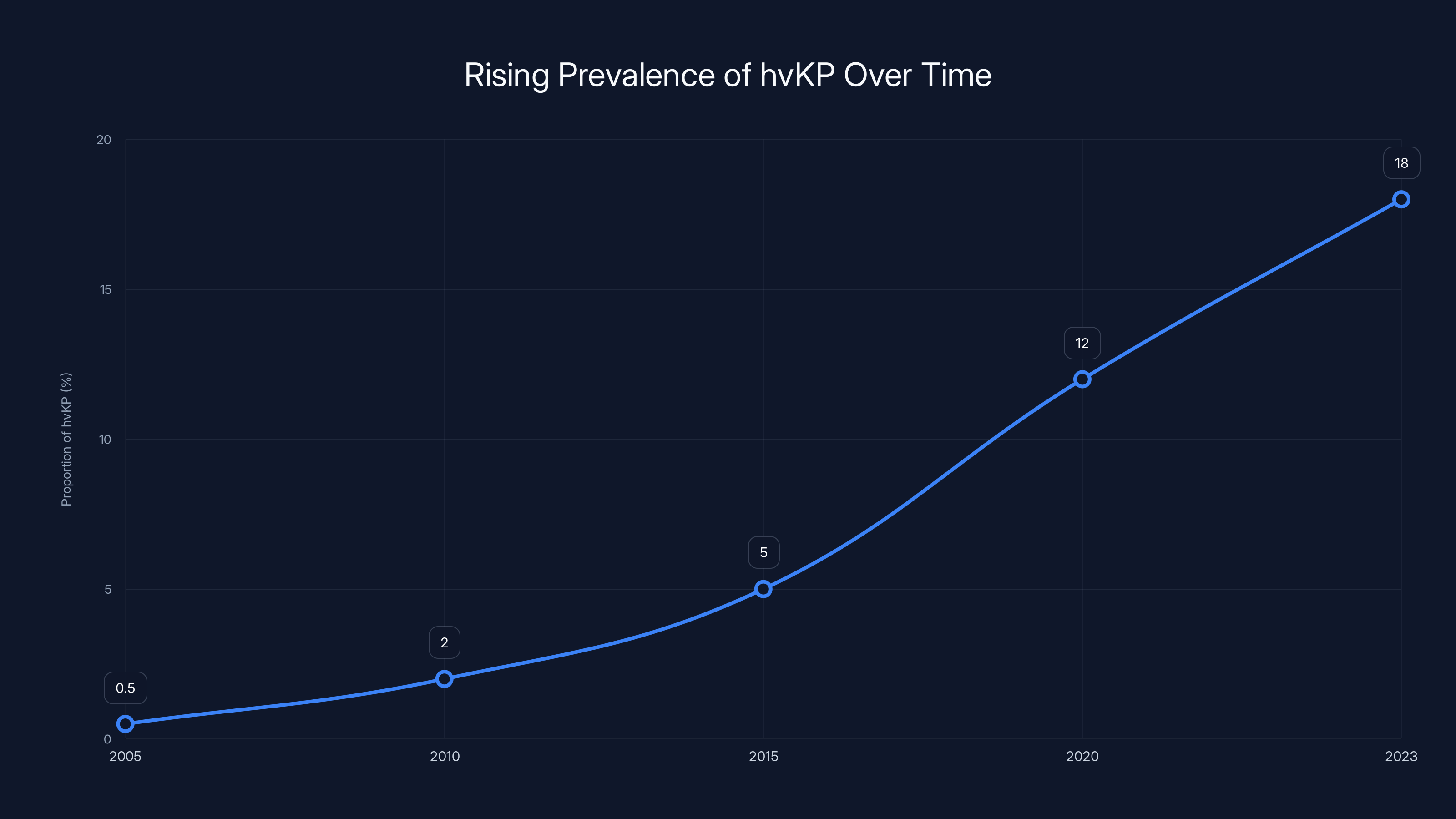
The proportion of hvKP among K. pneumoniae isolates has increased from near 0% in 2005 to an estimated 18% in 2023. This trend highlights the growing global concern over hvKP spread and its potential impact on public health. (Estimated data)
The Eye: An Unusual But Devastating Manifestation
Eye infections from bloodborne bacteria are uncommon. When they occur, they're typically in immunocompromised patients with high bacterial loads in the bloodstream. The eye is protected by multiple barriers: the blood-brain barrier (which also protects ocular tissues), the blood-retinal barrier, and the immune privilege of the eye.
However, hv KP's ability to achieve very high bacterial loads and its aggressive virulence factors can overcome these barriers. Endogenous endophthalmitis (infection seeded from the bloodstream) occurs in a subset of hv KP patients. When it does occur, the consequences are catastrophic.
The eye is a particularly vulnerable organ because once infection establishes within the vitreous humor (the gel in the back of the eye), antibiotics struggle to reach therapeutic concentrations. The eye has poor blood supply to the vitreous, and antibiotics don't penetrate well across the blood-retinal barrier. Additionally, the immune response within the eye is limited. The eye is immune-privileged, meaning it deliberately downregulates immune responses to avoid damage to delicate visual structures. This immune privilege that normally protects the eye from autoimmune damage becomes a liability when there's an active infection.
In endophthalmitis, the infection triggers a severe inflammatory response as the immune system attempts to clear the bacteria. The inflammation damages the retina, the optic nerve, and other vision-critical structures. Even if antibiotics ultimately kill all the bacteria, the inflammatory damage is already done. Vision is permanently lost.
Panophthalmitis, as seen in the New England case, is the most severe form of ocular infection. Every layer of the eye is involved in the inflammatory process. The extraocular muscles swell, preventing eye movement. The optic nerve is compressed and damaged. The retina is destroyed. The anterior and posterior segments are filled with pus and inflammatory cells.
In such cases, the eye typically becomes non-functional. Surgeons face a difficult decision: attempt to save the eye with aggressive antibiotics and possibly surgical drainage of the vitreous (vitrectomy), knowing the patient will likely be blind in that eye regardless, or remove the eye entirely. Removal eliminates a source of infection and eliminates the ongoing pain and inflammation, but it's a devastating procedure for the patient.
In the New England case, by the eighth day of hospitalization, the eye had progressed to such severe inflammation that there was no realistic chance of visual recovery. The eye was bulging out of the orbit due to the mass effect of the inflammation and abscess. The optic nerve was stretched and damaged. At that point, enucleation (surgical removal) was the appropriate choice.
Brain Involvement: Meningitis And Abscesses
The central nervous system is another organ that hv KP frequently targets. Like the eye, the brain is protected by specialized barriers: the blood-brain barrier (BBB). This barrier is incredibly selective about what molecules and cells it allows to pass. It's designed to protect the brain from pathogens, toxins, and other threats. It's also designed to prevent most antibiotics from reaching the brain in therapeutic concentrations.
For bacteria to cause meningitis or brain abscess, they must either:
- Achieve very high bacteremia levels that overwhelm the BBB's protective mechanisms
- Express specific virulence factors that allow them to cross the BBB
- Exploit damaged regions of the BBB caused by inflammation or other pathology
hv KP appears to accomplish all three. Its high virulence allows it to achieve very high bacteremia levels. It produces virulence factors that facilitate crossing the BBB. And the inflammatory response triggered by the initial infection can damage the BBB, allowing further penetration.
In the New England case, MRI revealed multiple lesions in the brain. Some of these likely represented early abscess formation. Others might have represented areas of meningitis or vasculitis (blood vessel inflammation). The presence of multiple lesions suggests that the bacterial dissemination was widespread and the immune system couldn't contain it.
Brain abscesses are a particular concern because they're difficult to treat. An abscess is a localized, walled-off collection of pus. While the wall of the abscess protects surrounding normal brain from the infection, it also limits antibiotic penetration. Only certain antibiotics achieve adequate concentrations within an established abscess. Additionally, if an abscess is large enough or in a critical location, it can cause neurological dysfunction through mass effect—simply by taking up space in a structure as confined as the skull.
In some hv KP cases, neurosurgery is necessary to drain brain abscesses. In other cases, antibiotic therapy alone is sufficient. The decision requires careful clinical judgment and often involves consultation with neurosurgery. In the New England case, the medical team decided against surgical drainage of the brain lesions, likely because they were either too small for practical drainage, too numerous, or in locations where surgery would carry excessive risk.

Pulmonary Manifestations: More Than Simple Pneumonia
The lungs are frequently involved in hv KP infection. The man in this case had over 15 nodules scattered throughout both lungs. This isn't typical pneumonia, where you might see consolidation in one or two lobes. This is disseminated lung disease from bacteremia.
When hv KP causes pulmonary infection, the pattern typically reflects bloodborne seeding rather than inhalation-based infection. The bacteria lodge in multiple locations throughout the lungs, causing small nodular infiltrates or even microabscesses. On chest X-ray or CT scan, you see what's called a miliary or nodular pattern: multiple small opacities distributed throughout the lung fields.
This pattern is different from what you'd see with aspiration pneumonia or community-acquired pneumonia caused by organisms like Streptococcus pneumoniae or Haemophilus influenzae. Those infections typically cause lobar or focal consolidation. hv KP's nodular, disseminated pattern reflects the systemic nature of the infection.
In patients with hv KP, the lungs are rarely the primary problem. They're secondary to hepatic infection. Once the liver abscess is established and continuously seeding bacteria into the bloodstream, the lungs are an inevitable target. The high blood flow to the lungs and the large surface area of the pulmonary vasculature make the lungs an easy target for circulating bacteria.
Treating hv KP pneumonia requires treating the underlying source, typically the liver abscess. If you treat the pneumonia with antibiotics but don't address the liver abscess, the pneumonia will recur. The bacteria will keep circulating and keep reinfecting the lungs.
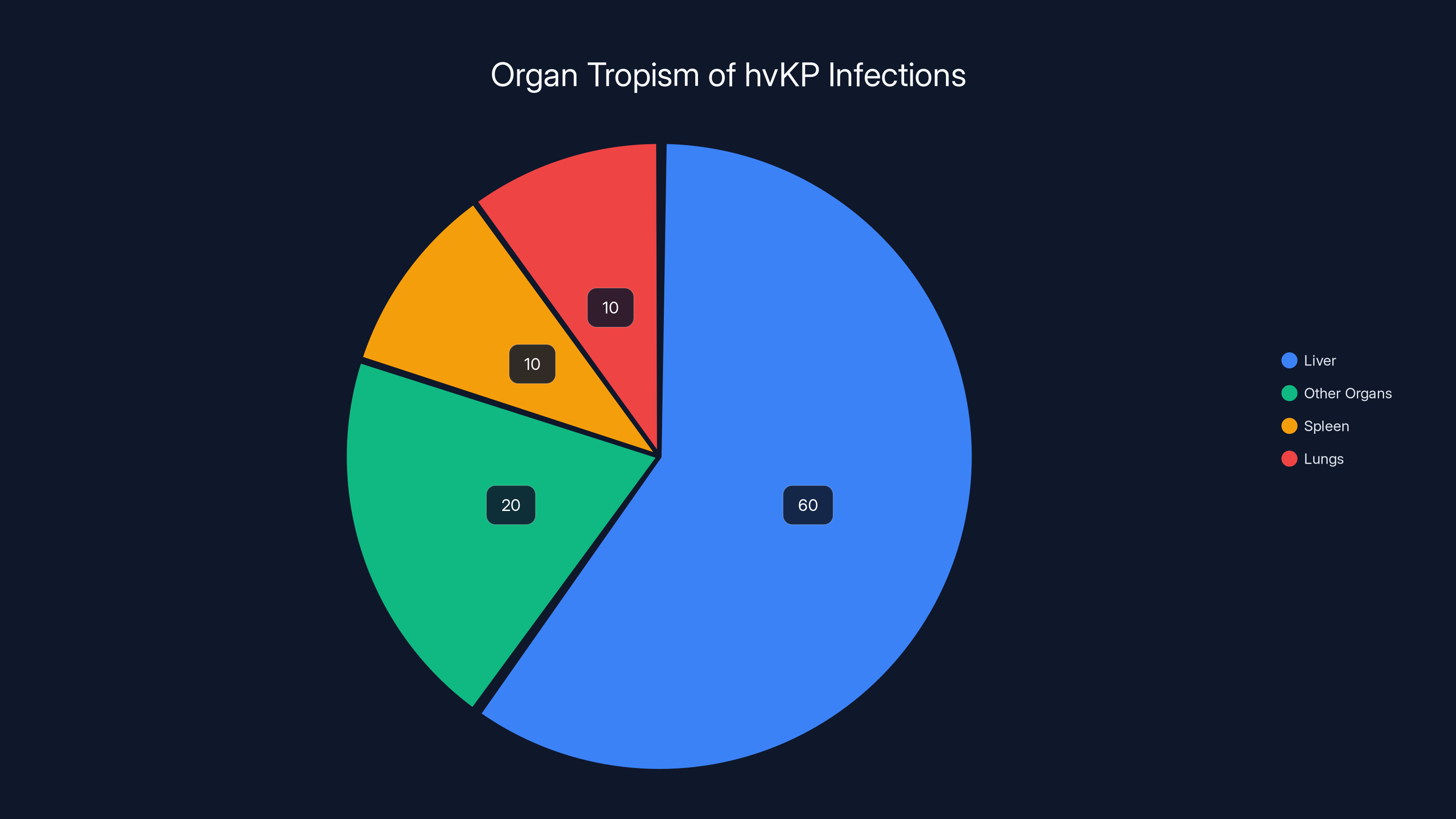
The liver is the primary target for hvKP infections, accounting for an estimated 60% of cases due to its vascular anatomy, nutritional environment, and unique immunological factors. Estimated data.
Hepatic Complications: Abscess Formation And Complications
As mentioned previously, liver abscess is the hallmark of hv KP infection. In the New England case, the patient had a single large abscess measuring 8.6 centimeters. In other cases, patients may have multiple abscesses, sometimes dozens throughout the liver.
Liver abscess formation follows a predictable pathophysiology. The hv KP bacterium, circulating in the bloodstream, lodges in the liver. It multiplies rapidly, overwhelming local immune defenses. Hepatocytes (liver cells) die from the infection and the inflammatory response. Immune cells accumulate, trying to contain the infection. The result is a collection of pus surrounded by a wall of inflamed tissue and granulation tissue.
The abscess grows larger as more bacteria multiply and more pus accumulates. If untreated, the abscess can rupture into the peritoneal cavity, causing bacterial peritonitis. It can rupture into the biliary system, potentially causing septic cholangitis. It can rupture into the bloodstream, causing bacteremia and sepsis.
From a treatment perspective, liver abscess in hv KP requires aggressive management. Antibiotics alone are often insufficient, particularly for large abscesses. The antibiotic must penetrate into the abscess, which is difficult because the abscess wall is relatively avascular (lacking in blood supply). Penetration of antibiotics into the abscess interior is often only 30-50% of serum concentrations.
For this reason, percutaneous drainage of large liver abscesses is often recommended. A radiologist, guided by ultrasound or CT imaging, places a drainage catheter into the abscess percutaneously (through the skin). Pus is drained, reducing the bacterial load and removing the source of ongoing bacteremia. Once drainage is established, antibiotics can work more effectively.
In some cases, the abscess is too extensive or too complicated for simple drainage. The abscess might be multiloculated (divided into multiple chambers by septa), making drainage incomplete. In such cases, more extensive surgical intervention might be necessary, up to and including partial hepatic resection in rare cases.
In the New England case, the medical team apparently decided against drainage of the hepatic abscess. This decision likely reflected the belief that antibiotic therapy would be sufficient, or perhaps that the abscess was in a location where percutaneous drainage carried excessive risk. The exact reasoning isn't clear from the case report.

Antibiotic Treatment: Finding The Right Drug
Once hv KP infection is recognized, the next critical step is identifying which antibiotics will work. This is where culture and susceptibility testing becomes essential. The bacterium is cultured from a sterile source (blood, abscess fluid, spinal fluid, etc.), and then the laboratory tests its susceptibility to various antibiotics.
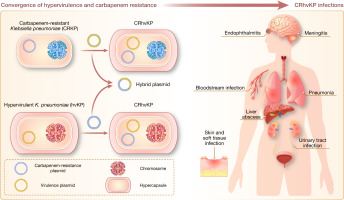
Historically, K. pneumoniae was universally susceptible to a wide range of antibiotics. Third-generation cephalosporins, fluoroquinolones, aminoglycosides, and carbapenems all worked. Resistance was uncommon. This made K. pneumoniae a relatively easy infection to treat from an antibiotic perspective.
However, in recent years, resistance in K. pneumoniae has become increasingly common. Many K. pneumoniae strains are now resistant to fluoroquinolones. Some have developed extended-spectrum beta-lactamase (ESBL) production, making them resistant to cephalosporins. Worst of all, some hv KP strains have acquired carbapenem resistance, which is a serious problem because carbapenems are often the last-resort antibiotic for resistant Gram-negative bacteria.
Carbapenem-resistant hv KP is a particular concern because it leaves few options. Colistin is sometimes used, but it's highly nephrotoxic (kidney-damaging). Some resistant strains are susceptible to tigecycline, but data on its effectiveness in hv KP infection are limited. Treatment of carbapenem-resistant hv KP infections can be challenging.
In the New England case, susceptibility testing indicated that the hv KP isolate was susceptible to certain antibiotics. The exact drugs aren't specified in the available case details, but presumably the medical team selected an appropriate antibiotic regimen based on the susceptibility results. Antibiotic selection in hv KP is crucial because inadequate antibiotic coverage can lead to treatment failure.

Clinical Outcome: When The Eye Can't Be Saved
Despite appropriate antibiotic therapy, some complications in hv KP infection are irreversible. The eye in the New England case had progressed to such severe panophthalmitis that blindness was inevitable. By the eighth day of hospitalization, surgical removal (enucleation) was the appropriate treatment.
This raises an important clinical point: recognizing hv KP early and starting effective therapy quickly is crucial. Every day of delay allows the infection to spread further and cause more damage. Once irreversible damage has occurred—such as retinal destruction or optic nerve necrosis—no antibiotic can reverse it.
The overall prognosis for hv KP infection varies depending on when diagnosis is made and how aggressively it's treated. Cases recognized early, with appropriate antibiotics started promptly and adequate source control (drainage of abscesses, etc.), have reasonable survival rates. Cases recognized late, with extensive disseminated disease, have much poorer outcomes. Mortality rates in reported series range from 5% to 30%, depending on the population studied and whether source control procedures were performed.
In the New England case, the patient ultimately survived the infection, though at the cost of his right eye. From a clinical perspective, this is actually a favorable outcome. The infection was controlled. The brain lesions resolved or stabilized. The liver abscess was treated. The lungs recovered. But the eye could not be saved.
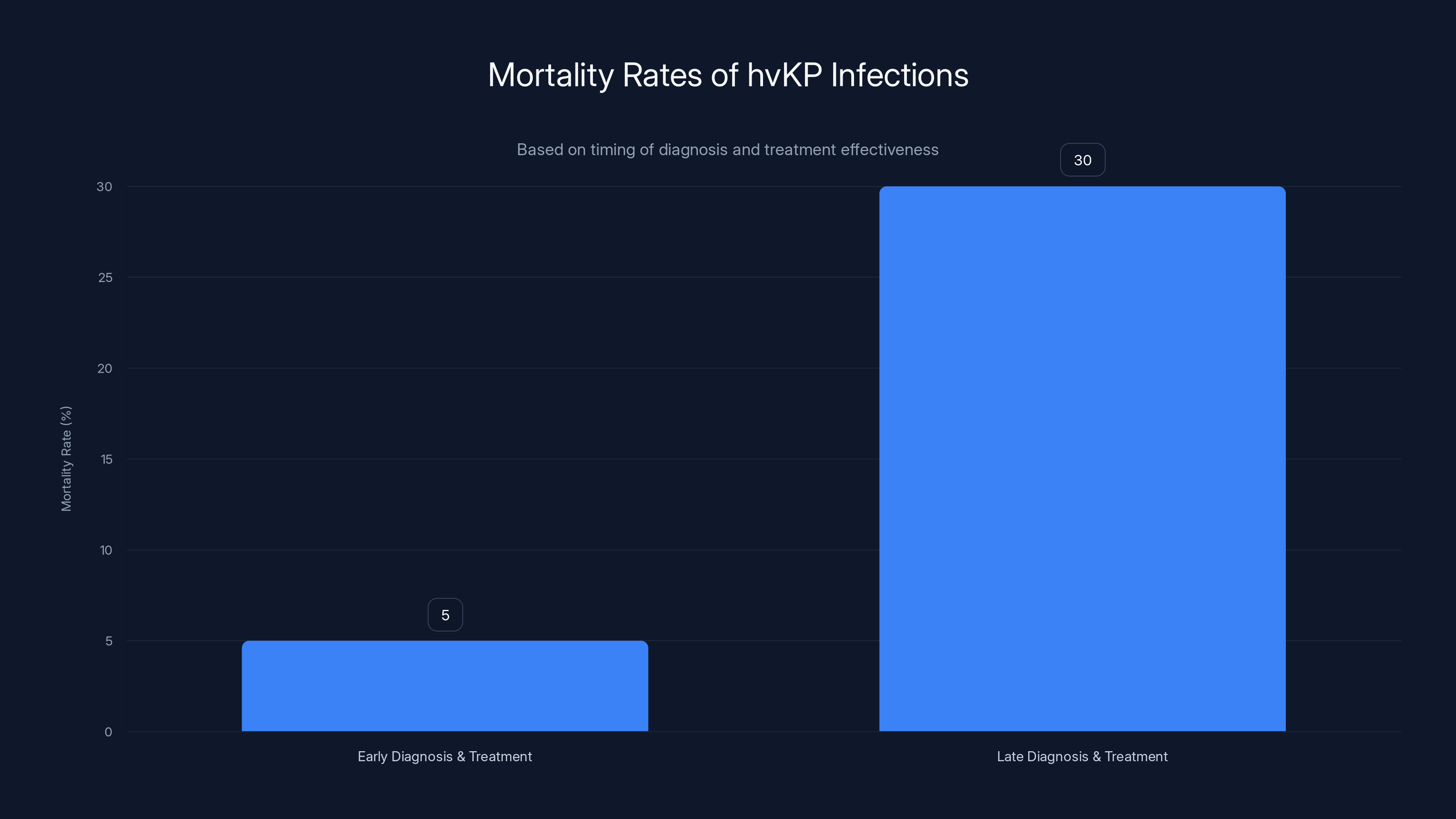
Mortality rates for hvKP infections can range from 5% with early diagnosis and treatment to 30% with late intervention. Early recognition and aggressive treatment are crucial for better outcomes.
Global Epidemiology: hv KP Around The World
Where did hv KP come from, and how is it spreading? The origin appears to be Asia, particularly East Asia. The first published cases in the medical literature came from Taiwan and other parts of the region in the 1980s and 1990s. The exact mechanism of emergence is unknown—it likely involved acquisition of plasmid-encoded virulence genes by a classical K. pneumoniae strain, followed by selective pressures favoring the hypervirulent variant in a specific population or geographic region.
From Asia, hv KP has spread to other continents. Cases have been reported in North America since the early 2000s. European cases have been documented. South American cases have been identified. Cases have been reported in Africa. The bacterium is clearly spreading globally.
The mechanism of spread likely involves multiple routes:
International travel: Infected individuals traveling between countries can carry hv KP in their intestinal tract and transmit it to others.
Contaminated food imports: Food contamination in one country can spread the organism to another country through international trade.
Healthcare worker transmission: In healthcare settings, cross-transmission can occur, particularly if infection control practices are inadequate.
Water contamination: In areas with suboptimal water treatment, contaminated water can serve as a source of exposure.
The frequency of hv KP isolation appears to be increasing. In surveillance systems that track K. pneumoniae isolates, the proportion that are hypervirulent (based on virulence gene detection) has been increasing over time. In some regions, hv KP now represents 5-20% of all K. pneumoniae isolates, up from near 0% just 10-15 years ago.
This rising prevalence is concerning for several reasons. First, hv KP causes more severe disease than classical K. pneumoniae, so increasing prevalence means more severe infections overall. Second, the potential for hv KP to spread resistance mechanisms—including carbapenem resistance—to other bacteria is a serious concern. Third, the unpredictability of hv KP (it affects healthy people without warning) makes it difficult to implement targeted prevention strategies.

Recognition And Early Detection: The Key To Survival
Survival in hv KP infection depends heavily on early recognition and prompt treatment. What features should raise suspicion for hv KP?
Severe liver abscess in a healthy person: If you see a patient with no significant risk factors presenting with a large liver abscess, hv KP should be on your differential diagnosis.
Metastatic presentation: If a patient has simultaneous involvement of liver, lungs, brain, and other organs, think hv KP.
Absence of typical risk factors: Classical K. pneumoniae infects hospitalized, immunocompromised, or surgery patients. hv KP infects healthy people. If you see a previously well person with serious K. pneumoniae infection, suspect hv KP.
Rapid progression: hv KP infection progresses quickly. A patient can go from feeling fine to critically ill in days to weeks.
Gastrointestinal precursor: A history of gastrointestinal illness (food poisoning-like symptoms) followed by systemic illness weeks later is suggestive of hv KP.
Endophthalmitis or panophthalmitis: While rare, the presence of endogenous eye infection (not from trauma or surgery) strongly suggests hv KP, especially if there's evidence of metastatic disease elsewhere.
Once hv KP is suspected, the string test can be performed rapidly if the organism has been isolated in culture. This provides relatively quick confirmation without waiting for genomic testing. Simultaneously, susceptibility testing should be performed to guide antibiotic selection.
Prevention: Can We Stop hv KP Before It Spreads?
Prevention of hv KP infection is challenging because the source is often contaminated food or water, which can be difficult to identify and control. There's no vaccine against hv KP. Individual measures that may reduce risk include:
Food safety: Proper cooking and food handling reduce risk of food-borne pathogen exposure. This is particularly important for foods that are commonly contaminated with K. pneumoniae, such as seafood and other high-moisture foods.
Hand hygiene: Standard hand hygiene practices reduce transmission of gastrointestinal pathogens, including hv KP.
Water safety: In regions where hv KP may be present in water supplies, boiling water or using appropriate filtration can reduce exposure.
Healthcare settings: In hospitals, appropriate infection control measures (hand hygiene, contact precautions for patients with hv KP) can reduce healthcare-associated transmission.
At a population level, surveillance systems that track the prevalence and spread of hv KP are important for understanding the epidemiology and potentially identifying sources of outbreaks. Some countries have begun to include hv KP in their antimicrobial resistance surveillance programs.
Future Directions: Research And Clinical Management
As hv KP continues to spread and cause more cases of severe infection, research efforts are focusing on several areas:
Rapid diagnostics: The goal is to develop a rapid, accurate test that can identify hv KP within hours rather than days. This could allow faster initiation of aggressive therapy and appropriate isolation precautions.
Vaccine development: Researchers are exploring whether a vaccine targeting hv KP virulence factors could prevent infection or reduce severity. This is challenging because effective vaccines require understanding which antigens elicit protective immunity.
Novel antibiotics: As resistance emerges, there's a need for new antibiotics effective against hv KP, particularly carbapenem-resistant strains. Several novel agents are in development.
Pathogenesis studies: Understanding exactly how hv KP establishes infection, overcomes immune defenses, and causes metastatic disease could lead to novel therapeutic approaches.
Epidemiological tracking: Genomic epidemiology can help track the spread of hv KP and identify specific strains and resistance mechanisms, potentially guiding public health responses.
FAQ
What exactly is hypervirulent Klebsiella pneumoniae (hv KP)?
Hypervirulent Klebsiella pneumoniae is a variant of the common bacterium K. pneumoniae that carries additional genetic material (usually on plasmids) encoding virulence factors that make it far more aggressive than classical K. pneumoniae. While classical K. pneumoniae typically infects hospitalized or immunocompromised patients, hv KP readily infects healthy individuals, causing metastatic disease involving multiple organ systems.
How is hv KP different from classical K. pneumoniae?
The key differences are virulence and host specificity. Classical K. pneumoniae is an opportunistic pathogen that primarily infects vulnerable patients in healthcare settings. hv KP has enhanced virulence factors including a thicker mucoid capsule, improved iron acquisition systems, and other factors that allow it to infect healthy people and establish systemic infections. hv KP characteristically spreads from the gut to establish large liver abscesses, then disseminates to lungs, brain, eyes, and other organs.
What causes hv KP infection to spread to so many organs?
The metastatic spread of hv KP reflects both its high virulence and the anatomy of how it enters the body. hv KP typically enters through food contamination, penetrating the intestinal barrier and entering the bloodstream. It has particular tropism for the liver, where it establishes large abscesses that continuously seed bacteria into circulation. From there, the highly virulent organism overcomes the barriers that normally protect organs like the brain and eye, establishing secondary infections in multiple sites.
How is hv KP diagnosed?
Diagnosis requires isolating the organism from blood, body fluid, or abscess cultures and then performing additional testing to confirm hypervirulence. The string test (examining if bacterial colonies form a string of mucoid goo when touched with an inoculation loop) is a simple bedside test that can suggest hv KP. Definitive diagnosis requires genetic testing to identify virulence genes. The challenge is that standard laboratory identification systems cannot distinguish hv KP from classical K. pneumoniae.
Can hv KP infections be treated?
Yes, hv KP infections can be treated with appropriate antibiotics selected based on susceptibility testing. However, treatment often requires more aggressive measures than classical K. pneumoniae infections. Large liver abscesses may need to be drained percutaneously to improve antibiotic penetration. When hv KP spreads to the brain or eye, the outcome can be devastating despite appropriate antibiotics—the inflammatory damage may be irreversible by the time treatment begins. Early recognition and prompt treatment are critical.
What is panophthalmitis and why is it so serious?
Panophthalmitis is infection involving all layers and structures of the eye. Unlike simple endophthalmitis (infection of the internal eye fluids), panophthalmitis involves the sclera, extraocular muscles, orbital tissues, and all intraocular structures. The severe inflammation associated with panophthalmitis causes irreversible damage to the retina and optic nerve, resulting in permanent blindness. In cases of severe panophthalmitis, surgical removal of the eye is often necessary.
Is there a vaccine for hv KP?
There is currently no vaccine for hv KP. Vaccine development is challenging because the virulence factors that define hv KP haven't been fully characterized in terms of which would elicit protective immunity. Research into vaccine development is ongoing, but no vaccine is available for clinical use at this time.
How can hv KP infection be prevented?
Prevention focuses on reducing exposure to contaminated food and water through proper food handling, cooking, and hand hygiene. In healthcare settings, standard infection control practices (hand hygiene, isolation precautions) can reduce transmission. There is no specific chemoprophylaxis available for prevention of hv KP in exposed individuals.
Conclusion: A Harbinger Of Emerging Threats
The case of the New England man with hypervirulent Klebsiella pneumoniae is more than just a dramatic medical story. It's a window into how infectious diseases evolve and spread in our modern world. A bacterium that was once confined to Asia, that caused primarily hospital-acquired infections in immunocompromised patients, has transformed into a global threat that can devastate previously healthy individuals without warning.
What makes this transformation so medically significant is that it wasn't driven by antibiotic resistance alone. hv KP isn't dangerous because it's resistant to drugs, though some resistant strains do exist. hv KP is dangerous because it's inherently more virulent. It's a stronger enemy, equipped with biological weapons that allow it to overwhelm the defenses of even a healthy immune system.
The metastatic nature of hv KP infection creates a uniquely challenging clinical scenario. Unlike many bacterial infections that can be managed by treating the primary site, hv KP requires identification and control of all infected sites simultaneously. The liver abscess must be addressed. The lungs must be treated. The brain lesions must be monitored. The eye, as we saw in this case, may already be too damaged to save.
The clinical team managing the New England patient did everything right. They recognized the unusual presentation. They worked through the diagnostic puzzle systematically. They identified the pathogen. They started appropriate antibiotics. They consulted specialists. Yet despite all this, the patient lost his eye. This sobering reality underscores that even excellent medical care can't always reverse the damage caused by hv KP once the infection becomes disseminated.
Looking forward, the increasing prevalence of hv KP globally demands vigilance from the medical community. Emergency physicians, internists, infectious disease specialists, and laboratory professionals need to maintain a high index of suspicion for hv KP when they see unusual presentations: metastatic infection in healthy people, liver abscess without typical risk factors, endogenous eye infections, or brain lesions without an obvious source.
The simple string test—a test so basic it requires nothing more than a culture plate and an inoculation loop—could be the difference between early recognition and delayed diagnosis. Minutes and hours matter in hv KP infection. The sooner appropriate antibiotic therapy and source control measures are implemented, the better the chance of preventing irreversible organ damage.
For patients and the general public, the key message is awareness. hv KP is not common, but it's not rare enough to ignore. If you experience gastrointestinal illness followed weeks later by fever, cough, or eye problems, seek medical evaluation. If you're diagnosed with a serious K. pneumoniae infection, ask whether hv KP testing has been performed. If you work in healthcare, stay informed about emerging infectious diseases in your region.
The story of hypervirulent Klebsiella pneumoniae is ultimately a story about how the microbial world evolves, adapts, and sometimes surprises us. The bacteria that most experts considered a solved problem, a relict of the pre-antibiotic era, has returned in a new and more dangerous form. Our response must be equally evolved: rapid recognition, aggressive treatment, and ongoing surveillance to track this emerging threat. The New England patient's case, tragic as it is, serves as a reminder of what happens when we're caught unprepared.
Key Takeaways
- Hypervirulent Klebsiella pneumoniae (hvKP) is a weaponized variant that infects healthy people, unlike classical K. pneumoniae which targets vulnerable patients
- hvKP causes metastatic disease by spreading from the gut to establish liver abscesses, then disseminating to lungs, brain, eyes, and soft tissues
- The string test—measuring if bacterial mucoid stretches >5mm from a colony—can rapidly suggest hvKP in culture without waiting for genetic testing
- Panophthalmitis from hvKP causes irreversible blindness and often requires surgical eye removal despite antibiotic therapy
- Early recognition and aggressive treatment including both antibiotics and source control (abscess drainage) offer the best chance of survival in hvKP infection
Related Articles
- Best Budget Earbuds Under $30: JBL Vibe Beam Review [2025]
- DDR5 RAM Prices Stabilize at $900: What It Means [2025]
- OpenAI Ads in ChatGPT: Why Free AI Just Got Monetized [2025]
- Trump and Governors Push Tech Giants to Fund Power Plants for AI [2025]
- Wavlink WL-UTD58 Thunderbolt 5 Dock Review [2025]
- EPA Rules xAI's Natural Gas Generators Illegal: What It Means [2025]

