![NIH-CDC Leadership Crisis: Inside the Dual Role Controversy [2025]](https://tryrunable.com/blog/nih-cdc-leadership-crisis-inside-the-dual-role-controversy-2/image-1-1771618117596.jpg)
The Unprecedented Double Agency Leadership: What You Need to Know
When you run one major federal health agency, you're already stretched thin. Running two? That's practically unheard of in American public health governance. Yet here we are in 2025, watching a single person attempt to oversee both the National Institutes of Health and the Centers for Disease Control and Prevention, the two most critical agencies responsible for disease research and disease prevention in the United States.
Jay Bhattacharya, a health economist with a medical degree, now holds both positions simultaneously. His appointment to lead the CDC comes as acting director following a dramatic reshuffling under Health Secretary Robert F. Kennedy Jr., whose tenure has already reshaped federal health policy in ways that would have seemed impossible just two years ago. This dual role isn't merely unusual. It's unprecedented in modern public health administration and represents a fundamental departure from how these agencies have operated since their establishment.
The arrangement has immediately drawn fierce criticism from researchers, public health officials, and former federal health leaders. They're not just concerned about the workload. They're worried about what his appointment signals about the current state of these agencies and about the direction of American public health policy under the current administration. Because this isn't just a story about one person getting a promotion. It's a story about institutional collapse, ideological takeover, and the consequences when crucial federal agencies lose operational leadership during a moment when measles is resurging, chronic disease rates are climbing, and vaccine hesitancy threatens herd immunity across the country.
What makes this story particularly alarming is the context. Under Bhattacharya's leadership at the NIH, the agency has experienced unprecedented institutional chaos. The budget freezes he oversaw, the mass defunding of clinical trials, the exodus of senior leadership—these aren't minor management issues. They represent a systematic dismantling of the nation's medical research infrastructure. Now, as he takes on the CDC role, experts are asking a simple question: if he can't effectively lead the NIH, what will happen when his attention is divided?
This article digs into the full scope of this crisis. We'll examine Bhattacharya's track record at the NIH, the leadership vacuum at the CDC, the political forces driving these changes, and what it all means for America's public health future. This is complicated stuff, but it matters. Your health depends on functional federal health agencies. Right now, those agencies are anything but functional.
TL; DR
- Dual Leadership Crisis: Jay Bhattacharya now directs both the NIH and CDC simultaneously, an unprecedented arrangement in federal health governance
- Chaotic NIH Tenure: Under Bhattacharya, the NIH froze $561 million in grants, defunded 304 clinical trials, and left 16 of 27 institutes without permanent directors
- Leadership Vacuum: Experts describe Bhattacharya as a "propagandist" rather than an operational leader, delegating most actual agency management to subordinates
- Vaccine Policy Concerns: Bhattacharya signed off on controversial CDC vaccine schedule changes and is expected to rubber-stamp further anti-vaccine initiatives
- Timeline Pressure: Bhattacharya can serve as acting CDC director only until March 25 under federal law, with no successor nominated yet

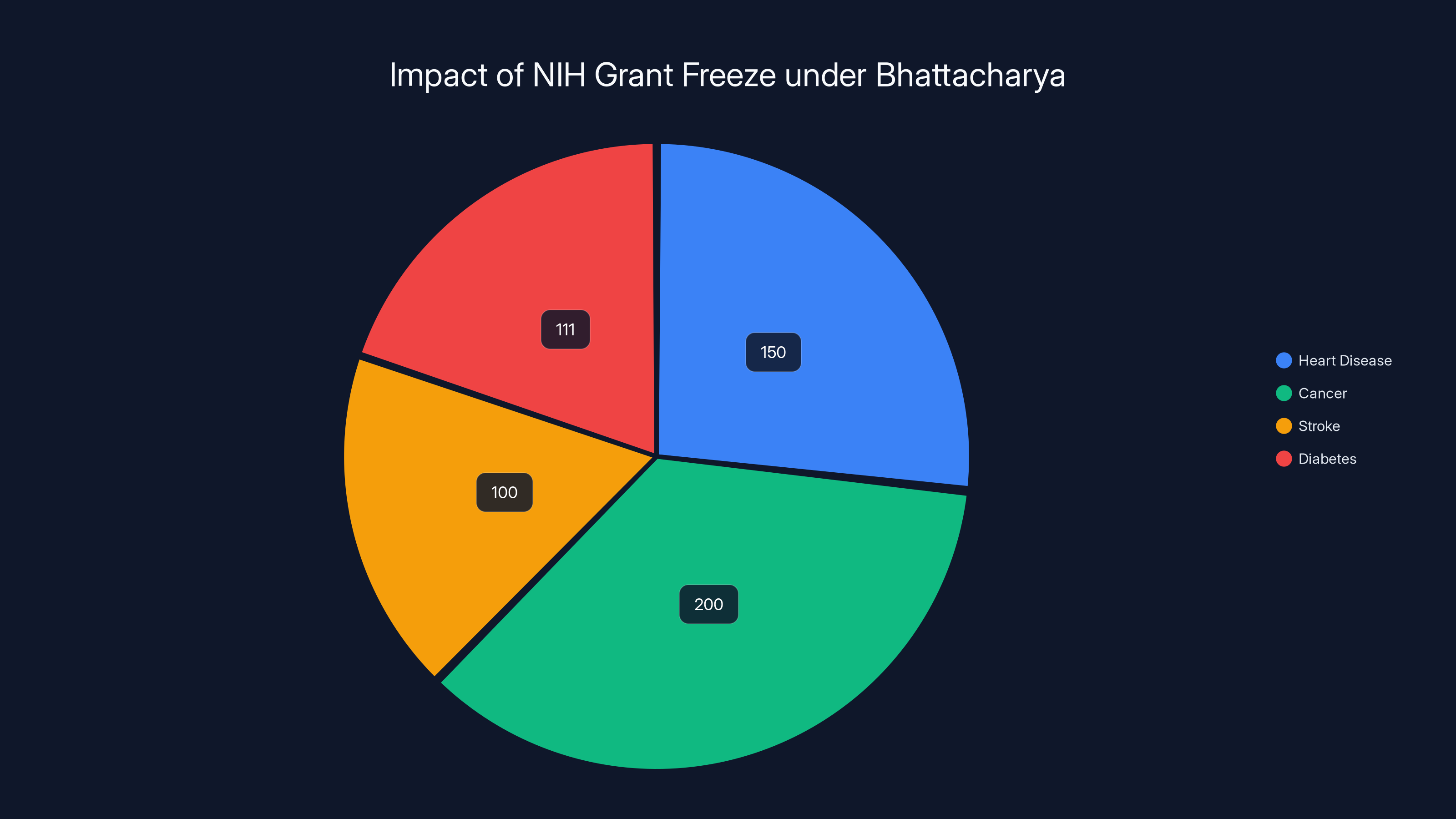
The NIH freeze under Bhattacharya affected $561 million in grants, impacting research on heart disease, cancer, stroke, and diabetes. Estimated data.
Understanding the NIH: America's Medical Research Engine
The National Institutes of Health is often called the world's premier medical research institution. This isn't hype. The NIH controls a budget of approximately $47 billion annually and funds roughly 300,000 researchers across the United States. If you've benefited from modern medicine in the last fifty years, there's a solid chance NIH-funded research played a role in that benefit.
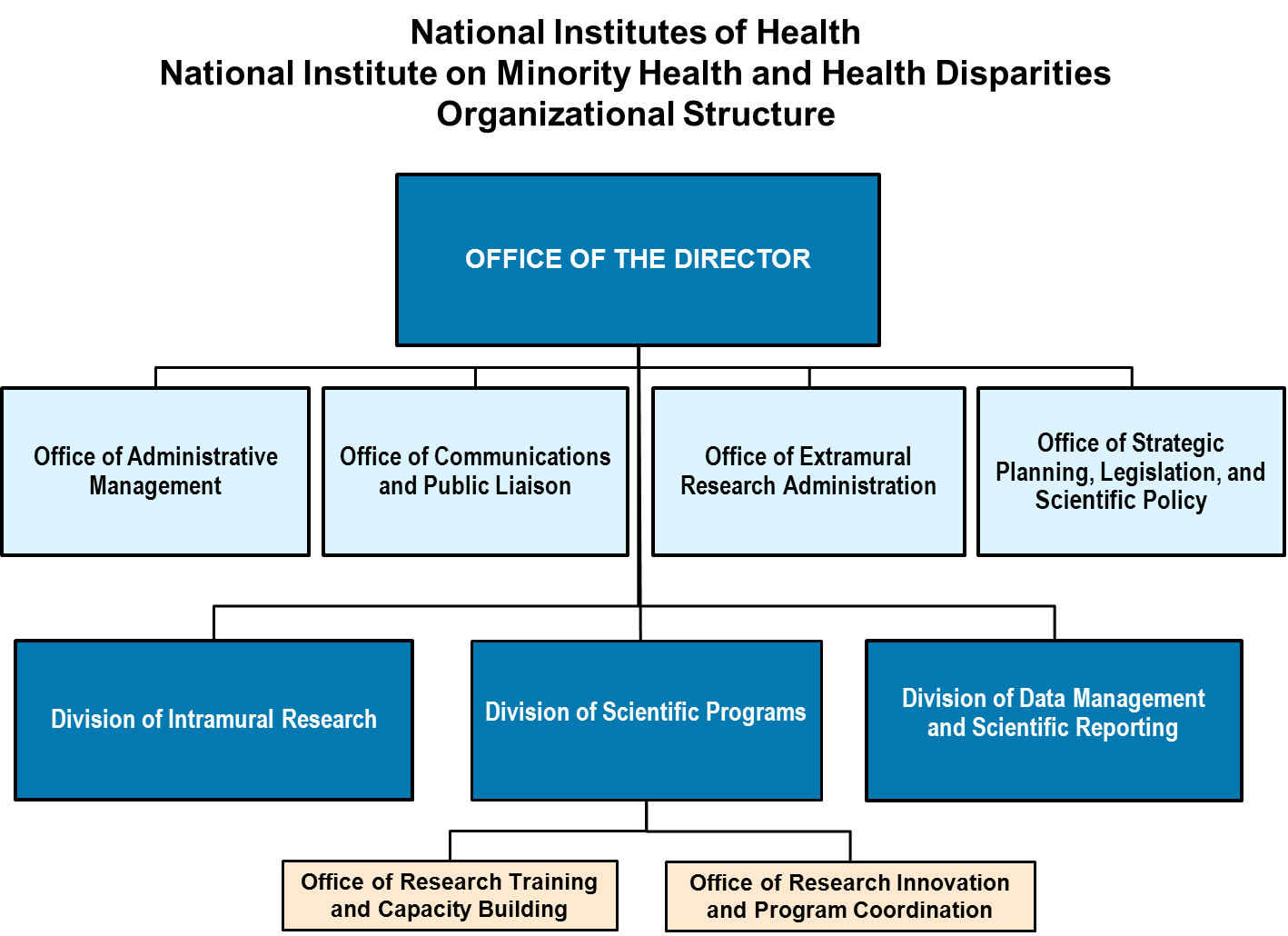
The agency operates through 27 separate institutes and centers, each focused on specific disease areas or research domains. The National Cancer Institute funds cancer research. The National Heart, Lung, and Blood Institute supports cardiovascular research. The National Institute of Allergy and Infectious Diseases manages infectious disease research. This structure allows specialized expertise while maintaining a unified federal research agenda.
Funding flows from the NIH to universities, research hospitals, and private research institutions across the country. A researcher at Johns Hopkins or Stanford who receives NIH funding is conducting federally supported research, but through their home institution. This decentralized structure allows the NIH to function as a funding engine rather than trying to conduct all research in-house.
The director role is critical because the director sets priorities, allocates budget, sets policy, and represents the agency to Congress and the public. When leadership is weak or absent, the entire system feels it. Researchers don't know which projects will be funded. Institutions can't plan. The research pipeline that produces tomorrow's medical breakthroughs slows or stops.
Understanding the NIH's role is crucial to understanding why Bhattacharya's leadership matters. When this agency stumbles, the consequences ripple through American medicine for years. Clinical trials get delayed. Young scientists lose funding and leave the field. Universities close research programs. Research centers in smaller cities and rural areas especially suffer because they're more dependent on NIH funding than major academic medical centers.
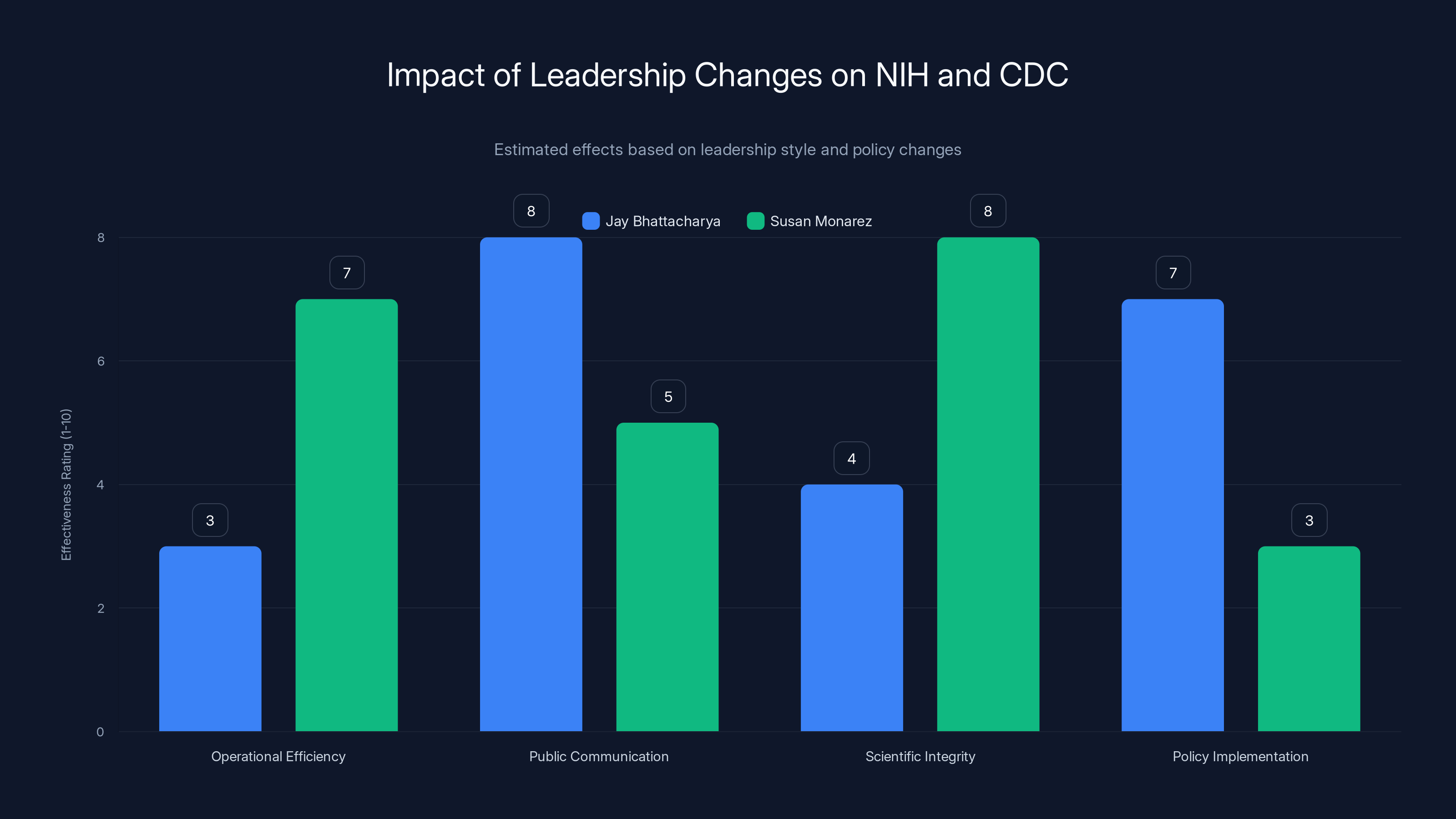
Estimated data suggests Bhattacharya excels in public communication and policy implementation, while Monarez was stronger in operational efficiency and scientific integrity.
The Centers for Disease Control: America's Disease Defense
If the NIH is the research engine, the CDC is the disease defense system. The Centers for Disease Control and Prevention is the nation's primary public health agency, responsible for disease surveillance, outbreak investigation, disease prevention recommendations, and public health emergency response.
The CDC operates differently than the NIH. While the NIH funds research elsewhere, the CDC employs thousands of epidemiologists, microbiologists, and public health specialists directly. These scientists are out in the field during disease outbreaks. They're tracking disease patterns. They're developing guidance that influences everything from vaccination schedules to hospital infection control protocols.
The director of the CDC sets policy that can affect 330 million Americans. Recommendations about which vaccines children should receive. Guidance about whether to quarantine during an outbreak. Decisions about which diseases to prioritize for prevention efforts. These aren't purely scientific matters. They're policy decisions with political consequences, which is why the CDC has become increasingly controversial in recent years.
The 2023 reform that made the CDC director a Senate-confirmed position (rather than just an appointed role) was meant to strengthen the agency's credibility. Senate confirmation requires vetting, and a director accountable to the Senate is theoretically more accountable to the public. Except there's a catch. The rule also imposed a limit: an acting director can serve only 210 days from the date the role became vacant. After that, the position must be filled either by Senate confirmation or... well, there is no "or." The position goes empty.
This legal structure becomes important later in our story, because it creates an artificial deadline for the Bhattacharya arrangement and forces difficult questions about whether the administration intends to nominate a permanent replacement.
The Leadership Shuffle: Three Directors in Months
The turnover at the CDC in 2024 and early 2025 has been nothing short of chaotic. Within roughly six months, the agency cycled through three different leaders, each representing a different approach and each ending in controversy or abrupt departure.
Susan Monarez arrived first. Monarez is a microbiologist with decades of federal health service and genuine respect in the public health community. She was brought in as acting director and ultimately became the first Senate-confirmed CDC director under the new 2023 rules. By all accounts, she knew the agency intimately and had credibility with both scientific staff and Congress.
Her tenure lasted approximately four weeks.
According to reporting, Monarez was ousted by Kennedy for refusing to rubber-stamp changes to vaccine recommendations proposed by Kennedy's advisors. These advisors are, by most accounts, overwhelmingly skeptical of vaccines and aligned with anti-vaccine activism. Monarez apparently drew a line. She wouldn't approve scientific policy changes that lacked scientific justification. Kennedy, impatient with this inconvenient insistence on evidence, removed her.
Enter Jim O'Neill. O'Neill's background is completely different from Monarez's. He's a Silicon Valley investor and entrepreneur with ties to Peter Thiel. He's not a public health scientist. He's not a career epidemiologist. He's a venture capitalist. Yet he was placed in the role of deputy secretary of HHS and then moved to lead the CDC.
O'Neill signed off on dramatic changes to the CDC's childhood vaccine recommendations. The agency slashed the recommended childhood vaccine schedule from 17 vaccines to 11, a change so significant and so unprecedented that it shocked the medical establishment. There is no scientific evidence supporting this reduction. Public health researchers and pediatricians raised alarms. But O'Neill approved it anyway.
Just like Monarez, O'Neill's tenure at the CDC was brief. He was reassigned, apparently to be nominated as director of the National Science Foundation (which was itself without leadership or a deputy director).
Now Bhattacharya. His appointment as acting CDC director represents a third approach: putting someone who technically has relevant credentials (he has both an MD and training as a health economist) into the role while presumably knowing he'll be more amenable to Kennedy's policy agenda than Monarez was.
The pattern is stark. Three leaders in roughly six months. Each change involves rapid departure of the previous leader. Each new leader appears to be selected partly for willingness to accept policy changes that would be scientifically controversial. This isn't normal leadership transition. This is leadership purge.
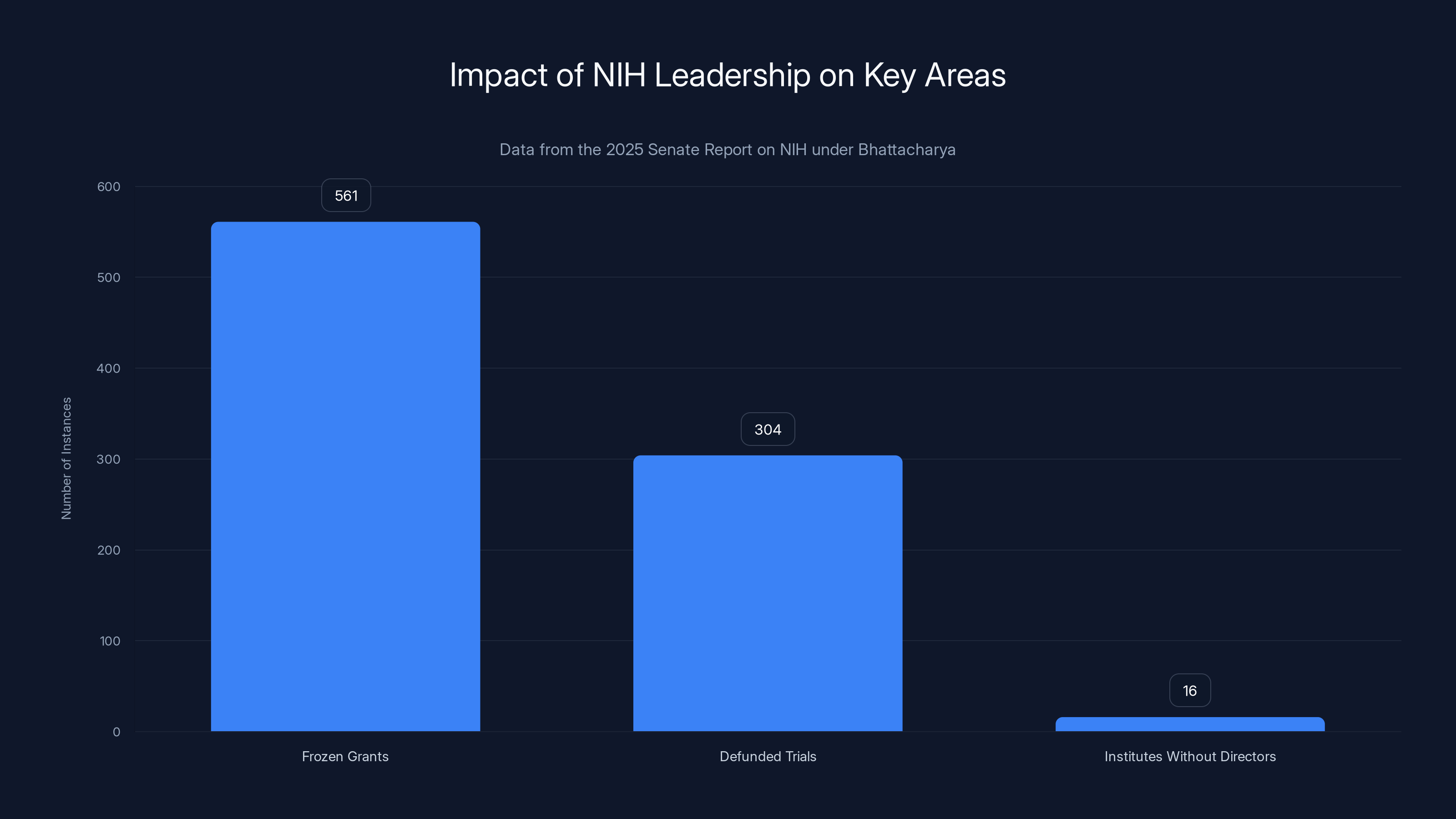
The Senate report highlights significant issues under Bhattacharya's NIH leadership, including 561 frozen grants, 304 defunded trials, and 16 institutes without directors.
Bhattacharya's NIH Track Record: Chaos by the Numbers
To understand what to expect from Bhattacharya at the CDC, you need to understand what his tenure at the NIH actually looked like. And the picture isn't pretty.
Start with the grants. The NIH's primary tool for advancing medical research is the research grant. These are competitive, peer-reviewed awards to scientists and research teams. Funding a grant doesn't mean the NIH is doing the research. It means the NIH is essentially betting that this research team, at this institution, working on this specific project, will produce valuable scientific knowledge.
Under Bhattacharya, the NIH implemented a freeze on certain categories of grants. According to a Senate report released in early 2025, this freeze touched $561 million in grants specifically designated for research on the four leading causes of death in America: heart disease, cancer, stroke, and diabetes.
Think about that. These are the diseases killing Americans at the highest rates. These are exactly the diseases where research funding could have the most impact. Yet the grants studying them got frozen. Why? The freeze appears to have been motivated by ideological concerns about the researchers involved or the institutions hosting the research, not by scientific merit.
Even more telling: at least 304 clinical trials were defunded. Clinical trials are where research turns into medical practice. They're where new treatments get tested in humans before approval. Defunding trials doesn't just waste previous research. It delays medical breakthroughs by years. It frustrates patient advocacy groups waiting for new treatments. It tells researchers that the NIH is no longer a reliable funding source.
The personnel situation is equally concerning. Of the NIH's 27 institutes and centers, 16 are currently operating without permanent directors. That's 59% of the institutes running headless. Some of these have never had vacancy rates this high. For comparison, during normal times, you might expect one or two institutes to be between directors during any given year, as people retire or move to other positions. Having 16 open is institutional crisis-level vacancy.
How does this happen? Mostly because Bhattacharya apparently isn't filling vacancies. Either nominations aren't being submitted, or nominees aren't being selected, or the selection process has stalled. The effect is the same: critical institute leadership positions sit empty, leaving acting directors to make decisions or, worse, no one clearly in charge.
Insiders report that Bhattacharya delegates most of his actual responsibilities to two senior officials. This might be fine if he were actively managing their work, providing guidance, and setting strategic direction. But by most accounts, that's not what's happening. Instead, Bhattacharya has become known for his extensive public appearances. He does podcasts. He gives interviews. He writes op-eds. This has earned him the nickname "Podcast Jay" among NIH staff and observers.
A nickname about someone being primarily a media presence rather than an operational leader is not a compliment.

The "Podcast Jay" Phenomenon: Leadership Through Media
The nickname "Podcast Jay" captures something important about Bhattacharya's approach to the director role. He's visible. He's articulate. He can explain science to general audiences. But visibility and effective leadership are different things.
Running a $47 billion federal agency requires making hundreds of decisions monthly. It requires building relationships with Congress, with scientific leaders across the country, with international health authorities, and with staff. It requires understanding the intricate politics of the NIH's 27 institutes and the delicate balance required to keep them all funded and moving forward.
Instead, sources describe Bhattacharya as heavily focused on his public profile. He's done numerous podcast appearances. He's written opinion pieces. He's done media interviews. This is valuable work in terms of public communication. But when done at the expense of actual agency management, it becomes a problem.
Jenny Norton is an NIH program officer who spoke to journalists anonymously about her experiences. She described Bhattacharya's approach bluntly: "He won't actually run the CDC. Just as he doesn't actually run NIH. His role for the administration, she added, is largely as a propagandist."
That's a harsh assessment. But it comes from someone inside the agency, actually working there, seeing how decisions get made.
Jeremy Berg is a former director of the National Institute of General Medical Sciences, one of the major NIH institutes. He expressed similar concerns: "Now, rather than largely ignoring the actual operations of one agency, he can largely ignore the actual operations of two."
Think about the implications. If Bhattacharya was already largely disengaged from day-to-day NIH operations, placing him in charge of the CDC as well doesn't make him more engaged. It makes the problem worse.

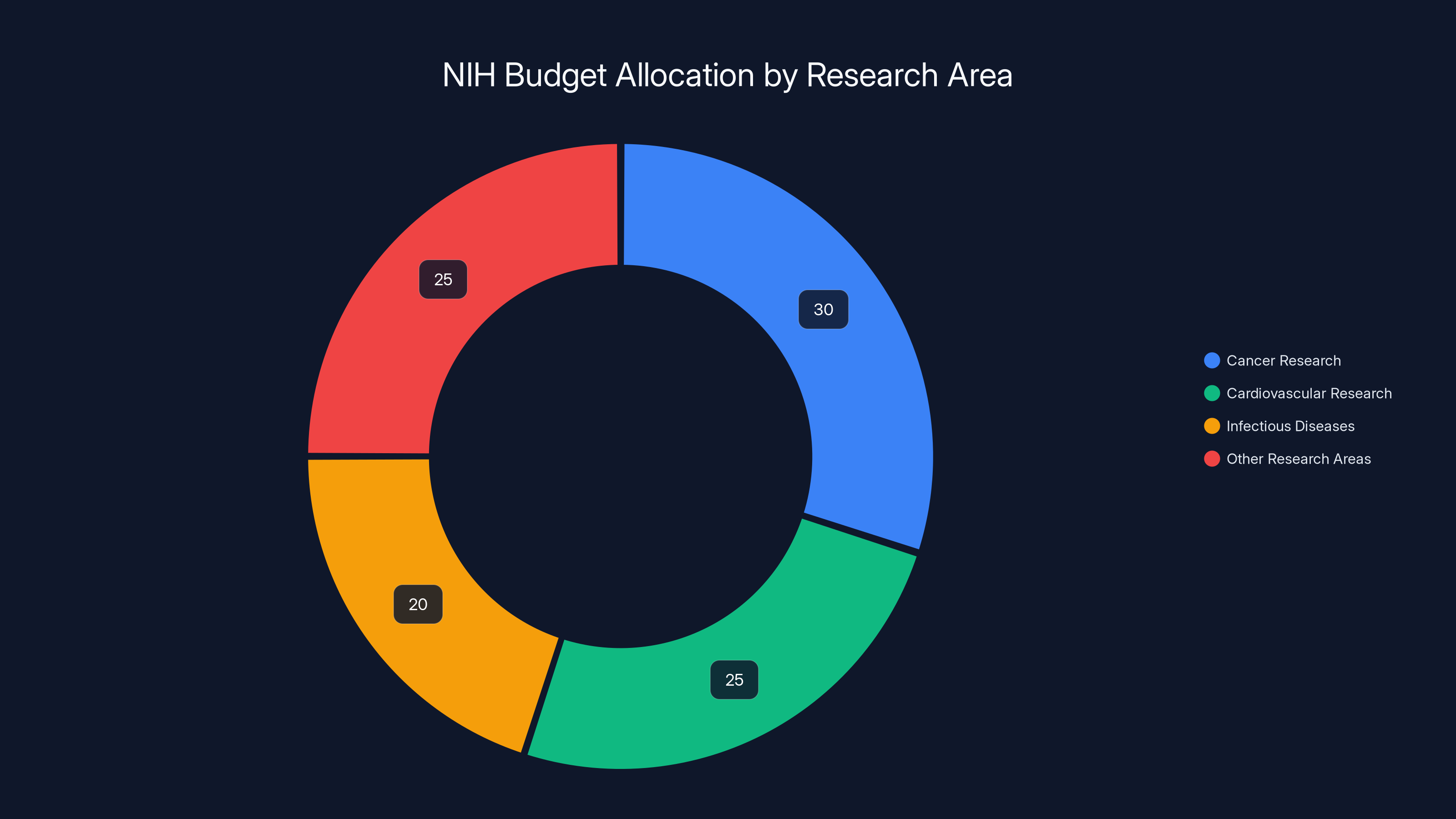
Estimated data shows a significant portion of NIH's budget is allocated to cancer, cardiovascular, and infectious disease research, reflecting their critical role in public health.
The Vaccine Schedule Overhaul: Dramatic Change Without Scientific Basis
One concrete policy action shows how Bhattacharya approaches controversial decisions: the CDC's vaccine schedule revision in 2024. This wasn't a minor adjustment. It was a dramatic, precedent-breaking change implemented without the scientific evidence typically required for such moves.
The childhood vaccination schedule has been refined over decades based on scientific evidence about which vaccines work best, when immunity develops optimally, and how to maximize protection. The current schedule recommends 17 different vaccines by age 18. These aren't random. They protect against diseases that kill or seriously injure children if not prevented.
In 2024, the CDC revised this schedule, reducing recommendations from 17 vaccines to 11. This wasn't done through the usual process of presenting evidence to the Advisory Committee on Immunization Practices (ACIP), getting expert review, and gradually implementing changes. It was done rapidly, with minimal scientific justification, apparently at the direction of Kennedy.
Bhattacharya signed off on this change. That fact matters because his signature represents implicit endorsement. As NIH director, his acceptance lent scientific credibility to a move that lacks scientific foundation. And it signals his willingness to approve policy changes driven by ideology rather than evidence.
Now he's moving to the CDC, where such decisions are his direct responsibility. If he approved vaccine schedule changes he didn't design and apparently didn't fully vet, what will happen when he has authority to directly set CDC policy?
Public health experts are expecting similar moves at the CDC. They predict that Bhattacharya will serve as a rubber-stamp for Kennedy's anti-vaccine agenda, just as O'Neill did. The pattern seems clear: Kennedy identifies the policy changes he wants, puts sympathetic people in positions to approve them, and lets them handle the logistics of implementation.

The Anti-Vaccine Alignment: What Drives This?
Understanding this story requires understanding Kennedy's ideological position on vaccines. Robert F. Kennedy Jr. has spent years promoting vaccine skepticism and anti-vaccine activism. He's written books questioning vaccine safety. He's associated with prominent anti-vaccine activists and organizations. His appointment as Health Secretary was shocking to much of the medical establishment precisely because of this history.
Kennedy isn't just skeptical about vaccines. He apparently wants to fundamentally reduce vaccine recommendations, restrict childhood vaccination, and shift federal policy away from promoting vaccines. This isn't a minor disagreement about which vaccines work best. It's a fundamental ideological commitment to reducing vaccination rates.
For this agenda to succeed, Kennedy needs people in key positions willing to implement it. Monarez apparently wasn't willing. O'Neill was. Bhattacharya has already shown willingness. So Kennedy is building an administration that shares his ideology and will execute his policy agenda.
This creates a conflict of interest. Public health policy should be driven by evidence about what protects public health. But if the people making policy are selected partly for ideological alignment, evidence becomes secondary. Policy becomes a tool for implementing a predetermined agenda rather than a tool for protecting public health.
The consequence is measurable. Measles, a disease essentially eliminated in the United States through vaccination, has started re-emerging. As vaccination rates drop (partly because of reduced recommendations and increased hesitancy), measles cases rise. This is not theoretical. It's happening now.

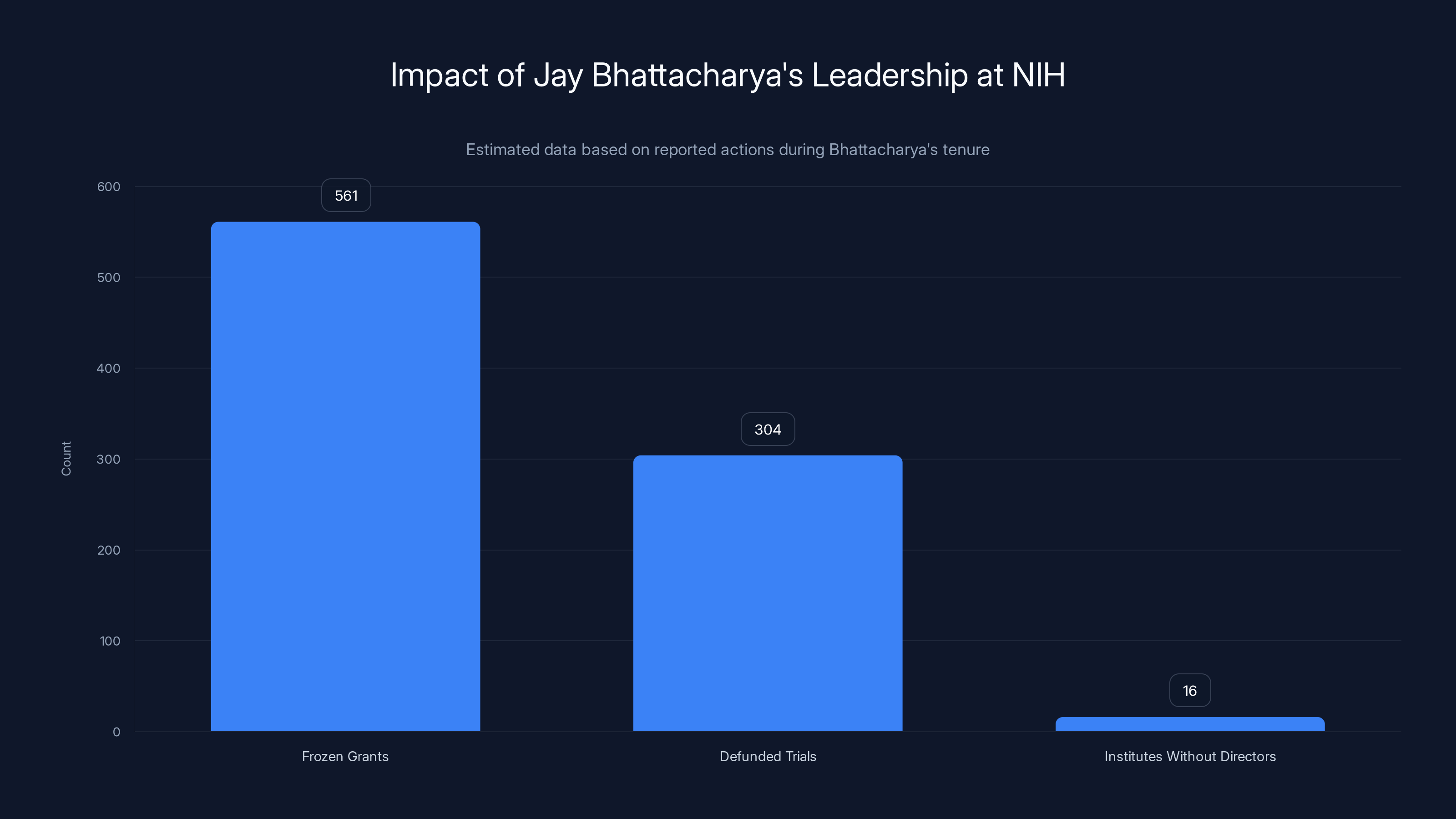
Jay Bhattacharya's tenure at NIH has seen significant disruptions, including the freezing of 561 grants and defunding of 304 clinical trials, leaving 16 institutes without permanent directors. Estimated data.
The Institutional Collapse: What Happens When Leadership Fails
When Bhattacharya took over the NIH, it was a functioning, if sometimes sclerotic, institution. Scientists could apply for grants. The grants could be funded. Research advanced. Progress continued.
Now, nearly a year into his tenure, the institution is visibly struggling. Researchers don't know which projects will be funded. Institutions can't commit resources. Grant awards have slowed. Young scientists are leaving the field because the funding is unreliable. It's not that Bhattacharya deliberately tried to collapse the NIH. It's that his leadership style and priorities don't match what the institution needs to function.
Kayla Hancock directs Public Health Watch, a nonprofit advocacy group focused on health policy. She's watched this unfold closely. Her assessment: "Jay Bhattacharya has overseen the most chaotic and rudderless era in NIH history, and for RFK Jr. to give him even more responsibility at the CDC is malpractice against the public health."
That's strong language, but it's hard to argue with the facts behind it. Sixteen institutes without permanent directors. $561 million in grants frozen. 304 clinical trials defunded. Senior scientists departing. That's not a successful tenure.
And now this person is being asked to take over the CDC. The timing couldn't be worse. The CDC is already reeling from the rapid leadership changes and controversial vaccine schedule revision. It needs stable, competent leadership. Instead, it's getting divided attention from someone whose track record at a sister agency is chaos.

The Senate Report: The Numbers Behind the Chaos
A Senate report released in early 2025 provided detailed documentation of what happened under Bhattacharya's NIH leadership. These aren't allegations or impressions. These are documented facts pulled from NIH records.
The $561 million in frozen grants across the four leading causes of death is just one datapoint. The 304 defunded clinical trials is another. The 16 institutes without directors is a third. Taken together, they paint a picture of an institution in crisis.
What makes the report significant is that it gives specifics. Researchers can point to specific grants that were frozen. Institutions can document specific trials that were defunded. Patients who were hoping for new treatment options can see exactly how their hopes got delayed. The report turns abstract concerns about leadership into concrete consequences for real people.
Senators from both parties expressed concern about the report's findings. This isn't a purely partisan issue. It's an issue about whether the NIH is functioning as intended. And by that standard, under Bhattacharya's leadership, it's not.
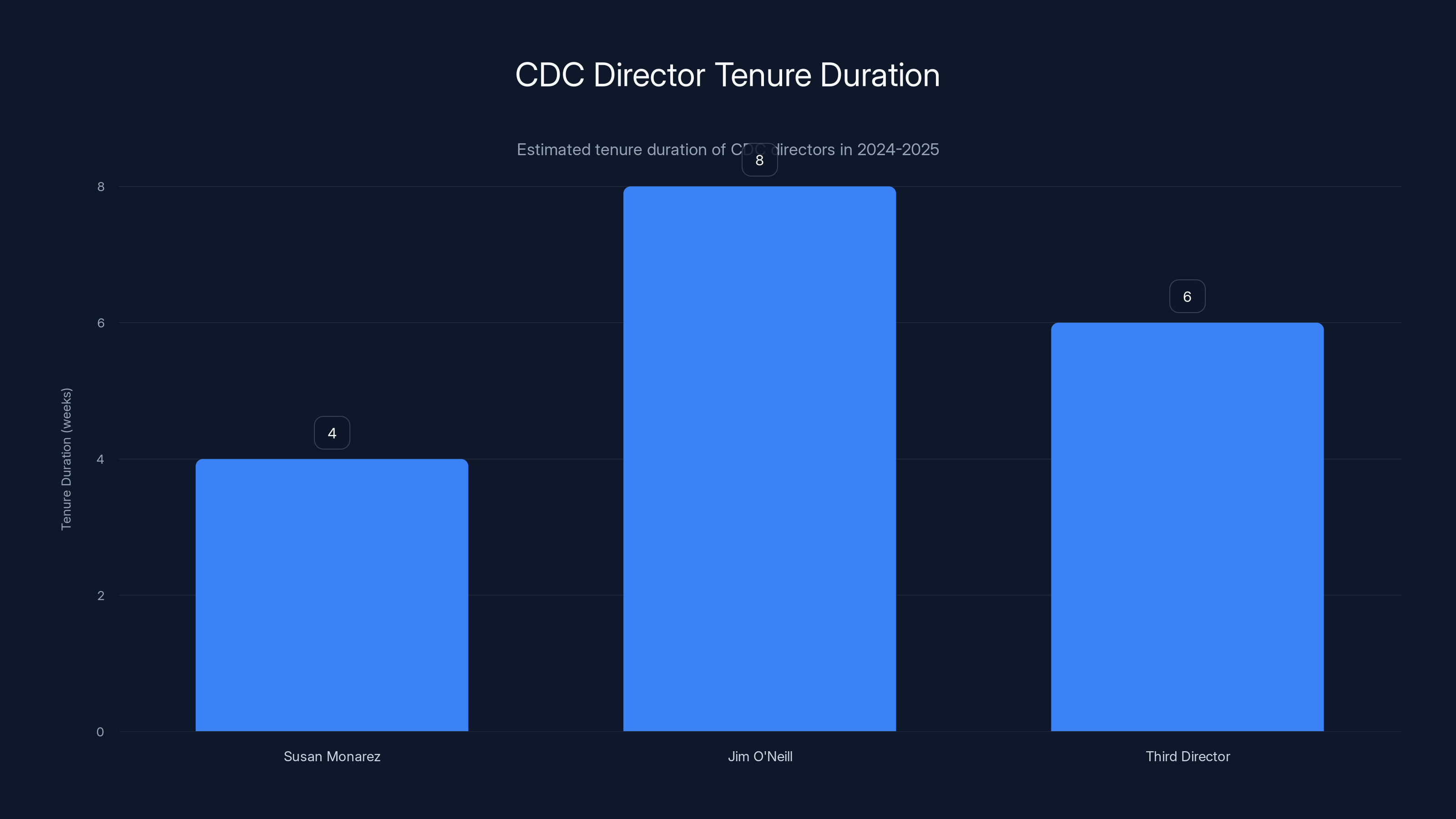
The CDC saw rapid leadership changes with directors serving short tenures, estimated between 4 to 8 weeks each, highlighting instability in leadership during 2024-2025.
The Timeline Pressure: The March 25 Deadline
Here's a wrinkle that adds urgency to this situation. Bhattacharya can serve as acting CDC director only until March 25, 2025. That's the deadline imposed by federal law for acting directors of CDC. It's 210 days from when the position became vacant.
After March 25, either a new Senate-confirmed director must be in place, or the position becomes legally vacant. There's no extension. There's no loophole. The law is clear.
President Trump has not nominated anyone for the role. There's no indication that a nomination is coming. Which creates an interesting question: what happens on March 26? Does the CDC director position simply go unfilled? Does Bhattacharya continue in some other capacity? Does someone new get rushed through Senate confirmation?
The deadline creates pressure. Either the administration needs to quickly nominate and confirm a new director (which would require Senate hearings, vetting, and floor debate), or it needs to figure out an alternative arrangement. Neither option seems politically easy given the controversy around Bhattacharya and given Senate skepticism about some of the administration's health policy directions.
This deadline creates a false sense of comfort for some observers. If Bhattacharya can only serve until March 25, maybe the damage is limited. But that's not quite right. Even a few months of problematic leadership at the CDC during a period of measles re-emergence and vaccine hesitancy is consequential. Disease outbreaks don't wait for leadership transitions.

The Broader Context: Public Health Under Siege
This story doesn't exist in isolation. It's part of a much larger pattern of challenge to federal health authority and to evidence-based medicine in general.
Measles is returning after decades of near-elimination. This isn't coincidence. It's consequence. Vaccination rates are dropping. As vaccination rates drop below the threshold needed for herd immunity, measles spreads. We're seeing this in real-time in multiple states.
Other vaccine-preventable diseases are similarly re-emerging. Whooping cough cases are rising. Mumps cases are rising. These are diseases we thought were controlled. We were wrong. They're coming back because immunity is dropping as vaccination rates drop.
Rubella, which we nearly eliminated, could re-emerge. The consequences would be measured in birth defects and miscarriages among pregnant women who lose immunity-through-vaccine.
This is happening while the CDC is in leadership chaos and the NIH is in institutional disarray. The timing could hardly be worse. We need strong, evidence-based public health leadership. Instead, we have divided attention and ideologically-driven decision-making.

Researcher and Expert Reactions: The Alarm is Widespread
Responses from the scientific and public health community to Bhattacharya's dual appointment have been swift and consistently critical.
Former CDC directors have expressed concern. Former NIH leaders have spoken out. Major scientific organizations have issued statements. The American Academy of Pediatrics, which represents 67,000 pediatricians, has raised alarm about vaccine policy changes. The American Medical Association has expressed concerns.
These aren't random critics. These are people who have led these institutions or led the professions that rely on them. They have credibility and expertise. Their concerns deserve attention.
What's particularly striking is how consistently they focus on the same issues: lack of operational leadership, willingness to approve policy changes without scientific justification, and apparent ideological commitment to reducing vaccination.
One former senior official described the situation as "institutional capture." The agencies haven't been destroyed. But they've been redirected toward serving a political agenda rather than a public health agenda. That's the real concern.

The Cascade Effect: How Problems at One Agency Hurt Another
When the NIH is in crisis, it doesn't just affect NIH researchers. It affects everything downstream. Hospital research programs that depend on NIH grants start laying off researchers. Universities postpone research facility construction. Young scientists decide not to go into research because funding is unreliable.
That damage takes years to reverse. A student who decides not to pursue a science Ph D because research funding is unreliable doesn't suddenly change their mind when funding stabilizes. They've moved on. Their talent is lost.
Similarly, when the CDC is in crisis, it affects everything that depends on the CDC. State health departments rely on CDC guidance. Local health departments rely on CDC surveillance data and recommendations. Hospitals use CDC protocols. Schools follow CDC guidelines. When the CDC is unstable and its guidance becomes unreliable, the entire public health infrastructure wobbles.
Add these effects together and you get what's happening now: federal health research is declining, public health guidance is confused, measles is re-emerging, and confidence in health institutions is eroding.

What's at Stake: The Consequences of Failed Leadership
This isn't abstract institutional politics. This is about real consequences for real people.
Parents trying to decide whether to vaccinate their kids now face confusion about what the CDC recommends. Is the reduced recommendation because these vaccines aren't safe? No—the science says they're safe. Is it because they don't work? No—they work very well. So why was the recommendation changed? Parents reasonably ask. And they don't get a clear answer because the answer involves political calculation rather than science.
Researchers with promising projects lose funding. Their work stops. The research team they were building disperses. The scientific progress they were making pauses. The patients hoping for new treatments wait longer.
Measles cases rise. Some children die. Some survive but have brain damage. Some will become deaf. These aren't hypothetical possibilities. These are documented consequences of measles infection. As vaccination rates drop, these consequences become more likely.
Healthcare workers at hospitals lose access to reliable CDC guidance. They have to make infection control decisions with less authoritative information. Outbreaks get worse. More people get infected. The healthcare system becomes less effective.
This is what failed federal health leadership looks like. It's not dramatic in the moment. But over months and years, it accumulates.

Looking Forward: What's Next?
The immediate question is who leads the CDC after March 25. Trump will have to nominate someone. That person will have to get through Senate confirmation. If Trump nominates someone similar to Bhattacharya or O'Neill, expect fierce Senate opposition. If Trump nominates someone with genuine public health credentials, Kennedy will probably object.
There's no obvious path forward that satisfies everyone. The fundamental tension remains: Kennedy wants to reduce vaccine recommendations and restrict vaccination. Most of the medical establishment opposes that. These positions are incompatible.
In the medium term, the question is whether the NIH and CDC can be stabilized. That requires getting permanent leadership in place. It requires filling those 16 vacant institute director positions. It requires restoring confidence in federal health institutions. That's a multi-year project that probably requires different leadership than currently exists.
In the long term, the question is whether federal health institutions can maintain their independence from political pressure while remaining accountable to elected government. That's a governance question that goes beyond any single administration. It's about what we expect from these institutions and how we structure them to meet those expectations.

The Institutional Memory Problem: Why This Matters More Than You Think
One thing that doesn't get enough attention in these discussions is institutional memory. Long-time CDC employees remember how measles was actually eliminated. They remember what the surveillance systems did that actually caught early cases. They remember why certain guidelines were written the way they were.
When leadership is chaotic, experienced people leave. They get hired away by other institutions. They retire. They leave the field entirely. And suddenly, the institutional knowledge about how to actually run a disease prevention agency walks out the door.
The next time there's a novel disease outbreak (and there will be), the CDC will be trying to respond with less experienced staff and less institutional memory of what actually works. That's a safety issue for the entire country.
FAQ
What is the significance of Jay Bhattacharya holding both NIH and CDC director positions simultaneously?
The dual role is unprecedented in modern public health administration and represents a major departure from standard governance practice. Both agencies are complex, $40+ billion institutions that require full attention from their leadership. The arrangement signals that the administration either can't find separate directors for both agencies, or is deliberately consolidating leadership under someone it trusts to implement its policy agenda. This creates immediate concerns about whether either agency will receive adequate operational attention.
Why was Susan Monarez removed as CDC director after just four weeks?
According to media reports, Monarez was ousted by Kennedy for refusing to rubber-stamp changes to vaccine recommendations that lacked scientific justification. Monarez apparently drew a line at approving policy changes that contradicted scientific evidence. Kennedy, seeking to implement his anti-vaccine agenda quickly, replaced her with someone more willing to approve such changes without scientific backing. This reflects a fundamental conflict between evidence-based public health and ideologically-driven policy.
What does "Podcast Jay" actually mean about Bhattacharya's leadership style?
The nickname reflects observations that Bhattacharya spends significant time on media appearances, podcasts, and public interviews rather than focused on day-to-day operational leadership of the NIH. Sources describe him as delegating most actual agency management to subordinates while maintaining a high public profile. This approach prioritizes public communication over institutional management, which can be effective for some leadership needs but leaves the actual operations of a complex agency understaffed and under-directed.
How did Bhattacharya's tenure at the NIH affect research funding?
Under Bhattacharya's leadership, the NIH froze $561 million in grants targeting the four leading causes of death in America and defunded at least 304 clinical trials. Additionally, 16 of the NIH's 27 institutes are operating without permanent directors, creating a vacuum in scientific leadership across the agency. These actions have slowed research progress, discouraged young scientists from pursuing research careers, and delayed potential medical breakthroughs.
What were the controversial changes made to the CDC's childhood vaccine schedule?
The CDC reduced childhood vaccine recommendations from 17 vaccines to 11 under O'Neill's leadership, a change that shocked the medical establishment. This wasn't done through the normal evidence-based process of presenting research to the Advisory Committee on Immunization Practices. Instead, it was implemented rapidly with minimal scientific justification, apparently at Kennedy's direction. The medical community, including the American Academy of Pediatrics, opposed the change because there's no scientific evidence supporting removal of the six vaccines.
What legal deadline constrains Bhattacharya's service as acting CDC director?
Federal law limits acting directors of the CDC to 210 days of service from when the position becomes vacant. This deadline falls on March 25, 2025, after which either a new Senate-confirmed director must be in place or the position becomes legally vacant. Trump has not nominated a replacement, creating uncertainty about CDC leadership after this date and forcing the administration to either quickly move a nominee through Senate confirmation or find an alternative arrangement.
How is measles re-emergence connected to these leadership changes?
Measles, essentially eliminated in the US through vaccination, is returning as vaccination rates drop. The drops result partly from reduced CDC vaccine recommendations and partly from increased vaccine hesitancy that results from public confusion about whether vaccines are actually necessary. With the CDC in leadership chaos and its guidance being questioned, it's struggling to communicate clearly about why measles vaccination is important, allowing the disease to re-emerge in communities with lower vaccination rates.
What are experts saying about the implications of this leadership crisis?
Public health experts, former agency leaders, and scientific organizations are expressing alarm about institutional collapse, lack of operational leadership, and willingness to implement policy changes driven by ideology rather than evidence. Former NIH leadership describes Bhattacharya as primarily a propagandist rather than an operational leader. Former CDC officials worry about the agency's ability to respond effectively to disease threats. The consistent message is that federal health institutions are being compromised at a time when strong leadership is essential.
How will this leadership instability affect the next disease outbreak?
When the next novel infectious disease appears (whether it's a new flu variant, an emerging pathogen, or another pandemic), the CDC will be responding with less experienced staff, less institutional memory, and less operational stability than it had before. This could slow response times, reduce effectiveness of surveillance and containment, and increase public confusion about agency guidance. The stakes are potentially very high for public health and national security.
What would it take to stabilize federal health institutions?
True stabilization would require appointing permanent, Senate-confirmed leaders to the NIH and CDC with genuine credentials and scientific standing. It would require filling the 16 vacant institute director positions at the NIH. It would require restoring evidence-based decision-making at both agencies. And it would require rebuilding staff confidence and institutional memory that has been damaged by rapid leadership changes. This is a multi-year project that probably requires different political leadership than currently exists.

The Path Forward: Rebuilding Trust and Function
Repairing federal health institutions won't happen quickly. Trust, once lost, takes time to rebuild. Institutional damage, once done, takes years to repair. The question going forward is whether the administration recognizes the problem and commits to fixing it, or whether the current trajectory continues.
What's clear is that the current arrangement can't be permanent. Two major federal health agencies can't be effectively led by one person whose time is divided and whose leadership style emphasizes public communication over operational management. The NIH can't function with 16 vacant institute director positions. The CDC can't effectively manage disease surveillance and prevention with unstable leadership.
The research pipeline that produces tomorrow's medical breakthroughs is already damaged. Young scientists are choosing other careers. Research institutions are scaling back programs. It will take conscious effort to rebuild that pipeline and restore confidence that NIH funding is reliable.
Similarly, the CDC's credibility as a public health authority is damaged. When the agency's vaccine recommendations seem driven by political ideology rather than scientific evidence, people reasonably become skeptical of what the CDC recommends. Rebuilding that credibility requires demonstrating genuine commitment to evidence-based decision-making.
The broader point is that federal health institutions matter. They're not just government bureaucracies. They're the infrastructure that prevents disease, advances medical science, and protects public health. When those institutions fail, everyone loses. It's not an abstract policy question. It's an issue with direct consequences for how many children get measles, whether promising research gets funded, and whether we're prepared for the next disease threat.
This story will continue to unfold. The March 25 deadline will force decisions. Trump will either nominate a new CDC director or not. Senate confirmation battles will likely happen if he does nominate someone. Meanwhile, the NIH will either continue under Bhattacharya's divided attention or new leadership will be brought in.
What matters is paying attention. Federal health leadership isn't sexy. It doesn't get cable news coverage most of the time. But it affects all of us, and we all have stakes in whether it functions effectively. That's why this story, for all its bureaucratic details and institutional complexity, matters to everyone with a family member who might someday need the benefits of medical research or disease prevention.

Key Takeaways
- Jay Bhattacharya holding both NIH and CDC director positions simultaneously is unprecedented and represents institutional governance failure
- Under Bhattacharya's NIH leadership, $561M in grants froze, 304 clinical trials defunded, and 16 of 27 institutes lost permanent directors
- CDC cycled through three directors in six months; removals correlate with unwillingness to approve anti-vaccine policy changes without scientific basis
- Vaccine schedule slashed from 17 to 11 recommended vaccines without scientific evidence, approved by leaders selected for ideological alignment rather than scientific expertise
- Measles re-emergence directly results from declining vaccination rates caused by reduced CDC recommendations and increased public vaccine hesitancy
- Experts describe Bhattacharya's leadership style as prioritizing public communication ("Podcast Jay") over actual operational management of complex agencies
- Federal law limits acting CDC director tenure to 210 days, creating deadline of March 25 with no successor nominated
- Institutional damage from rapid leadership changes and grant freezes will take years to repair, discouraging young scientists from research careers
- Public health agencies need stable, evidence-based leadership; current arrangements undermine credibility during critical period of disease re-emergence
Related Articles
- Ivermectin as Cancer Treatment: Why Federal Research Funding Raises Red Flags [2025]
- NIH's Second Scientific Revolution: COVID Anger, MAHA Politics, and Real Reform [2025]
- Measles Brain Swelling: South Carolina Outbreak and Encephalitis Risk [2025]
- HHS AI Tool for Vaccine Injury Claims: What Experts Warn [2025]
- South Carolina's Measles Outbreak Hits Record Breaking 789 Cases [2026]
- Political Language Is Dying: How America Lost Its Words [2025]

